- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
Carotid Cavernous Fistula (CCF)
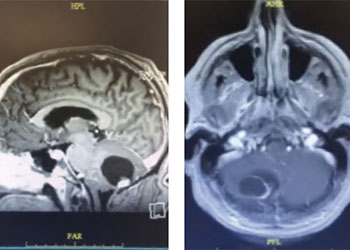
Cerebellar Hemangioblastoma
October 27, 2021
Man in 40’s with progressive confusion and headaches
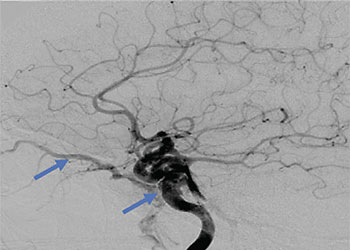
October 27, 2021Collateral venous drainage into the orbit and skull base was observed (Figure A). After successful cannulation of the direct aperture between the right carotid artery and the cavernous sinus, balloon-assisted coil embolization of the posterolateral compartment was performed until the fistula was closed (Figure B and C). He experienced immediate cessation of his pulsatile tinnitus with an early improvement of the right VI nerve palsy and near-complete recovery of his vision within 6 weeks



Figure: (A) Right ICA Cavernous Fistula with Venous Shunting (B) Balloon Assisted Coil Embolization (C) Fistula Cured Post Embolization
KEY LEARNING POINTS:
- Carotid-Cavernous Sinus Fistula (CCF) may occur because of traumatic or spontaneous communication in the walls of the intracavernous ICA or its branches directly to the cavernous sinus resulting in short-circuiting or shunting of high-pressure arterial blood into the venous system of the cavernous sinuses.
- Intra-cavernous aneurysms are often felt to predispose to a Direct CCF which has high rates of arterialized blood flow and can result in a rapid progression of clinical symptoms including cranial nerve injury and vision loss.
- Early evaluation by a neurovascular specialist is recommended for patients presenting with new-onset or progressive pulsatile tinnitus, especially in patients with associated visual symptoms or new neurologic deficits.
REFERENCE
Endovascular Techniques for Treatment of Carotid-Cavernous Fistula. Gemmete J Ansari S, Gandhi D. Journal of Neuro-Ophthalmology. March 2009 – Volume 29 – Issue 1 – p 62-71.
CATEGORY: ENDOVASCULAR // CAROTID CAVERNOUS FISTULA (CCF)
Carotid Cavernous Fistula (CCF)
A 59-year-old man who is otherwise healthy presented to his PCP with progressive right-sided pulsatile tinnitus for 4-6 weeks. His PCP and ENT evaluated him extensively and prescribed multiple courses of steroids and subsequent unremarkable MRI and MRA imaging. He developed acute onset diplopia secondary to a new partial right VI nerve palsy several days prior to our evaluation. A cerebral angiogram confirmed the presence of a high flow direct fistula of the right internal carotid artery–right cavernous sinus.