- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
Ruptured Thoracic Spinal Arterial Dissecting Aneurysm

Spinal Dural Fistula Causing Myelopathy & Incontinence: Reversal After Endovascular Embolization
October 27, 2021
Pituitary Tumor with Cushing’s Disease
October 27, 2021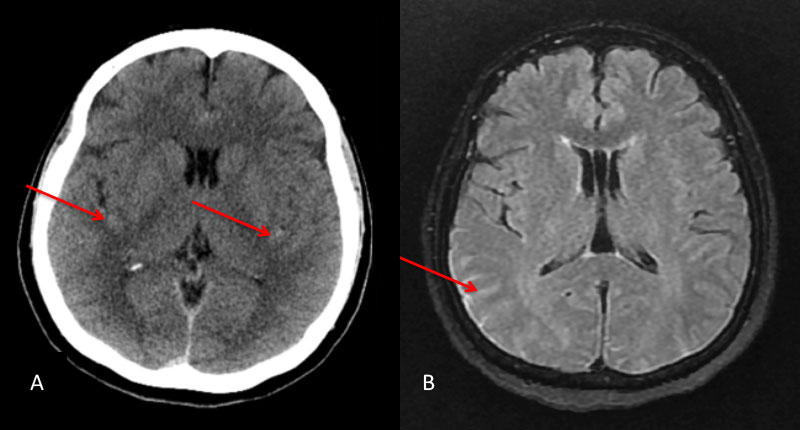
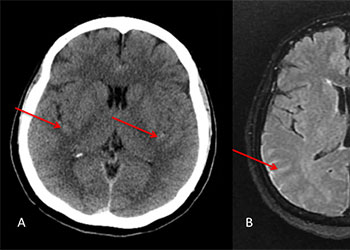
Figure 1: A) Non Contrast CT and B) MRI FLAIR studies demonstrate subtle Subarachnoid hemorrhage in the sylvian and parietal sulci (arrows)
The subararachnoid hemorrhage was focused primarily within the spinal axis of the cervical thoracic and lumbar spine with secondary extension into the brain. A suspicious focal hematoma or mass was observed within the left T4-T5 region with local mass effect representing an intradural extra medullary abnormality with secondary compression of the cord and central myelopathic T2 signal abnormality (Figure 2. A,B,C,D).
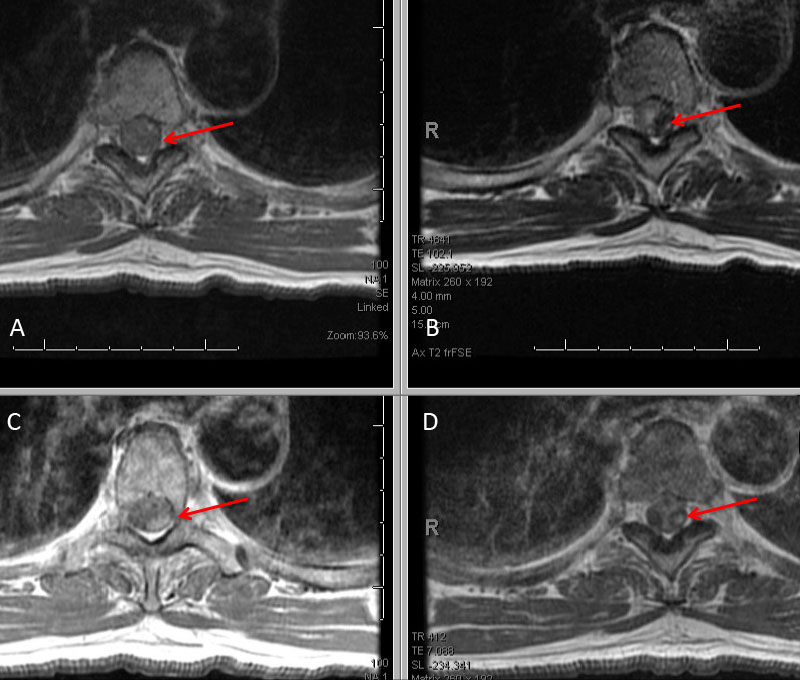
Figure 2: A) T1 B) C+ T1 C) STIR D) FS C+ T1 demonstrate focal hemorrhage, contrast enhancement, mass effect, and myelopathic cord signal at T4 (arrows)
His initial angiogram excluded an underlying aneurysm or high flow arterial venous malformation of the brain, however a dissecting aneurysm of the left T5 pedicle was malformation of the brain, however a dissecting aneurysm of the left T5 pedicle was identified extending into the left T4-T5 left paramedullary space (Figure 3. A).
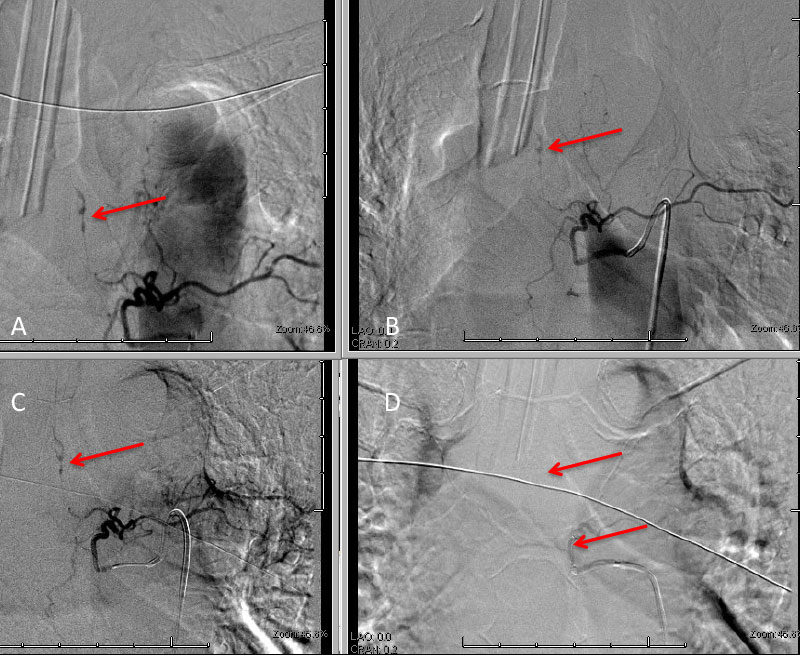
Figure 3: A) Initial left T5 DSA; B) 5 days post; C) Microcatheter DSA D) Post Coil Embolization demonstrating aneurysm obliteration
A selective WADA test of the left T5 pedicle with Brevital and lidocaine was performed and demonstrated loss of motor and sensory signal on intraoperative monitoring within the left lower extremity suggesting that this dissecting aneurysm of left T5 did have some contribution to the anterior spinal axis at this level. After initial discussions of options, we decided to initially place him on medical therapy with aminocaproic acid (72 hours), bed rest, and hemodynamic control of his blood pressure in the efforts to allow the aneurysm dissection to heal and potentially spontaneously thrombose. In addition, we volume expanded him in efforts to develop collaterals in the event that embolization of this dissection was required. A follow-up angiogram performed 5 days later demonstrated that the dissection did not thrombose and appeared very similar to the initial angiogram (Figure 3. B) and felt to represent a high risk for recurrent hemorrhage. We had extensive discussions with the patient and his spouse, who were prepared for potential difficult decisions regarding treatment of this high-risk lesion. Based on our judgment, we felt that the risks of recurrent hemorrhage were significant and that embolization of the feeding pedicle of left T5 should be performed to decrease the risk of potentially life-threatening or paralyzing disabling hemorrhage. We performed a coil embolization of the left T5 pedicle at the origin of the spinal artery, with the intention that collateral perfusion of the spinal cord would be achieved by adjacent healthy pedicles (Figure 3. C and D). He tolerated the procedure very well without adverse events or new neurologic deficits. We maintained the patient in the neuro ICU on bedrest with permissive hypertension and anticoagulation for 24-48 hours to encourage collateralization. After an additional 2 days of mobilization and observation, and a follow MRI demonstrating improved myelopathic signal and resolving focal left T4 hemorrhage, he was discharged home neurologically intact in good condition. Over the hemorrhage, he was discharged home neurologically intact in good condition. Over the next 6 weeks, his symptoms of abdominal and back pain resolved, and he regained all of his activities of daily living without limitation or neurologic deficits.
DISCUSSION:
Although rare, isolated spontaneous dissections and aneurysms of the anterior and posterior spinal artery axis have been described, presenting with a variety of clinical syndromes including subarachnoid hemorrhage, spinal cord ischemia, or local mass effect. The anterior spinal arterial axis has extensive contributions from the intracranial vertebral arteries, the artery of cervical enlargement (Lazorthes), to the artery of lumbar-sacral enlargement (Adamkiewicz) as well as radicular arteries (varying from 5- 9) of the cervical and thoracic segments. The natural history of these lesions remains unclear, with reports of spontaneous resolution, recurrent hemorrhage, enlargement, as well as morbidity with medical therapy. Surgical and endovascular approaches are considered in high-risk presentations, especially those presenting with SAH and neurologic deficits. Careful consideration to the location, vascular collateralization, functional testing, and risk-benefit analysis is required for each patient in these complex, rare, dangerous conditions (References 1-4).
REFERENCES:
- Romanes GJ. The Arterial Blood Supply of the Human Spinal Cord. Paraplegia. 1965 Mar;2:199-207. doi: 10.1038/sc.1964.37. PMID: 14261502.
- Massand MG, Wallace RC, Gonzalez LF, Zabramski JM, Spetzler RF. Subarachnoid hemorrhage due to isolated spinal artery aneurysm in four patients. AJNR Am J Neuroradiol. 2005 Oct;26(9):2415-9. PMID: 16219857.
- Berlis A, Scheufler KM, Schmahl C, Rauer S, Götz F, Schumacher M. Solitary spinal artery aneurysms as a rare source of spinal subarachnoid hemorrhage: potential etiology and treatment strategy. AJNR Am J Neuroradiol. 2005 Feb;26(2):405-10. PMID: 15709145.
- Etz CD, Kari FA, Mueller CS, Silovitz D, Brenner RM, Lin HM, Griepp RB. The collateral network concept: a reassessment of the anatomy of spinal cord perfusion. J Thorac Cardiovasc Surg. 2011 Apr;141(4):1020-8. doi: 10.1016/j.jtcvs.2010.06.023. PMID: 21419903; PMCID: PMC3062787.
CATEGORY: ENDOVASCULAR // RUPTURED THORACIC SPINAL ARTERIAL DISSECTING ANEURYSM
Ruptured Thoracic Spinal Arterial Dissecting Aneurysm
A man in his 60’s presented with acute onset of abdominal pain radiating to the back. The initial evaluation focused on GI abnormalities which were unremarkable. A screening CT scan of the brain was performed and suggested a possible subarachnoid hemorrhage which was subsequently confirmed on MRI and lumbar puncture (Figure 1A and 1B).

Authors
To learn more about the author, click his name or photo: