- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
Tale of Two Pathologies Contributing to Lumbar Stenosis with Spondylolisthesis
Great News for NSPC Patients – You’re Protected from Out of Network Bills
April 4, 2023
A Good Solution For Patients With Osteoporosis Who Need Surgery For A “Slipped Disc” or Spondylolisthesis
July 24, 2023
Fig 4
The actual structural cause of lumbar thecal sac compression can vary in degenerative spondylolisthesis and stenosis. The culprits are commonly thickened ligamentum flavum or severe facet arthropathy or a combination of both. If there is facet hypertrophy contributing to the stenosis, the facet angle and spinal level will dictate the relative contribution of the inferior or superior process to the stenosis. Because of its more anterior position, the superior articular process is more commonly involved in contributing to stenosis whether it be foraminal, lateral, or central stenosis. In certain cases the contribution of the inferior process might be more prominent depending on angle or vector of the slip or relative degree of hypertrophy. These two following cases illustrate a different preponderance of pathologies that contribute to stenosis in degenerative spondylolisthesis.
This 73 year-old female had a long history of low back pain and left thigh pain and heaviness of her legs when she ambulated or did activities. She failed all means of conservative treatment including epidurals and PT. On exam she had mild weakness of her left quad but otherwise was intact. Lumbar MRI (Fig 1) revealed significant L4-5 lumbar stenosis and a grade 1-2 spondylolisthesis. Her main pathology was severe, thickened “knobs” of ligamentum forming at the posterior margin of the superior facet processes of L5 and lamina (Fig 2). The patient underwent a decompressive laminectomy of L4 as well as removal of the inferior processes of L5 to widely decompress bilaterally the L4 and L5 nerve roots. Intraoperatively, the descending L5 nerve roots were compressed severely by this severe thickened ligamentum in the subarticular recess. Because of the significant spondylolisthesis we augmented her decompression with fusion. She underwent an L4-5 posterolateral fusion with segmental instrumentation (Fig 3)). Postoperatively she had an uneventful course with relief of her leg pain.

Fig 1: Sagittal T2-weighted lumbar MRI demonstrating grade 1-2 spondylolisthesis L4-5 with severe stenosis (red arrow)
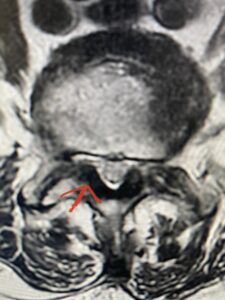
Fig 2 Axial T2-weighted lumbar MRI demonstrating severe lumbar stenosis at L4-5 secondary to thickened ligamentum flavum “knobs” (red arrow) contributing to central and lateral recess stenosis.

Fig 3: Lateral and AP fluoroscopic images demonstrating placement of pedicle screws for L4-5 fusion for spondylolisthesis.

Another patient is a 62 year-old female with progressive low back pain and right leg pain and numbness that radiates to the top of her foot. She tried physical therapy and epidural injections. MRI demonstrated severe L3-4 stenosis and a grade 1 spondylolisthesis (Fig 4). There was L5-S1 and L4-5 disc collapse with modic end-plate changes. Biomechanically because of the significant degeneration of these disc spaces which stiffened the L4-S1 segment more stress was placed on the L3-4 segment, resulting in significant premature degeneration and compensatory stenosis and segmental instability. The MRI also showed pathologically, because of the slip, the L3 inferior processes were more anteriorly oriented and hence contributing to the majority of the lumbar canal compromise. Note the more sagittally-oriented facets in this case compared to the prior case (Fig 5). The patient underwent a decompressive laminectomy with attention of removing the inferior processes of L3 to fully decompress the canal. We also performed an L3-4 fusion with instrumentation (Fig 6). The patient had an uneventful postoperative course with improvement of leg pain. Of note with relief of the disabling leg pain patients are generally very happy. Patients can often manage their low back pain; it is the leg pain that they just can’t tolerate.

Fig 4: Sagittal T2-weighted lumbar MRI demonstrating L3-4 grade 1 spondylolisthesis with severe stenosis (blue arrow)
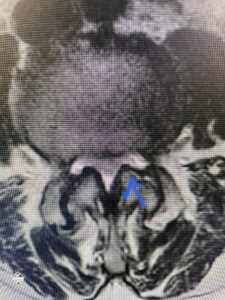
Fig 5 Axial T2-weighted lumbar MRI demonstrating significant L3 inferior facet contribution of severe stenosis (blue arrow)

Fig 6: AP and lateral fluoroscopic images demonstrating pedicle screw placement in L3-4 fusion for spondylolisthesis.


