- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
55 year old woman with one year of progressive hearing loss in the left ear / Acoustic Neuroma

Right Vertebral Artery Compression Syndrome
October 27, 2021
Symptomatic Near-Occlusion of the Carotid Artery
October 27, 2021Nomenclature: While these tumors are generally referred to as “acoustic neuromas”, it is understood that these are generally, in reality, “vestibular schwannomas”. The tumor arises from the eighth cranial nerve, the vestibulocochlear nerve, which transmits information regarding balance (the superior and inferior vestibular nerve fibers) and hearing (the cochlear or acoustic nerve fibers). These tumors arise from the vestibular nerves. Furthermore, these tumors arise from the nerve covering cells, the “schwann cells” not the neurons themselves. So while the tumors are usually called acoustic neuromas, the term “vestibular schwannoma” is technically more accurate.
Genetics: Acoustic neuromas develop spontaneously about 95% of the time. In these cases, there is no known cause. 5% of the time, acoustic neuromas develop as a result of a genetic condition call “neurofibromatosis type 2” or NF2. NF2 is transmitted in an autosomal dominant pattern, and causes the development of bilateral acoustic neuromas, as well as other tumors of the central nervous system.
Presentation: The most common symptoms of acoustic neuromas are unilateral hearing loss and tinnitus. The next most common symptom is decreased balance. Because MRI’s are now readily available, these tumors are generally discovered relatively early, when they are small. However, these tumors can become quite large and can cause significant compression of the brainstem which can result in more extensive symptoms.
Natural History: Over time, these tumors tend to grow slowly, but some can grow somewhat faster. Hearing usually decreases over time. Hearing loss can occur in a gradual manner, or in a stepwise manner, where there are sudden decreases or complete loss of hearing. These hearing declines may or may not recover.
Treatment options: Treatment options include (1) observation; (2) stereotactic radiosurgery; and (3) surgery. Observation is used for very small tumors or small-medium sized tumors that are stable over time. Surgery is used for very large tumors. Stereotactic Radiosurgery ( superfocused radiation treatments), particularly Gamma Knife, is used for most cases of acoustic neuromas. Unless the tumor is extremely large, Gamma Knife offers comparable control to open surgery / craniotomy, with a much lower risk profile.
Gamma Knife for Acoustic Neuromas: Gamma Knife involves a one day treatment. Patients undergo application of a head frame, receive an MRI of the brain, and then go into the Gamma Knife machine itself for about an hour. Local anesthetics and sedatives are provided for various portions of the procedure to optimize comfort during the procedure. Gamma Knife is about 95% successful at controlling tumor growth. A few patients who receive Gamma Knife for acoustic neuroma may ultimately require a second Gamma Knife treatment, or rarely surgery. Gamma Knife will maintain hearing at the current level about 60-70% of the time.
Technical Aspects of Gamma Knife Treatment: Dose to the tumor is set to 12-13 Gy to the edge of the tumor. The 50% isodose line is set to the edge of the tumor. Dosing under 12Gy is less effective at tumor control, and dosing over 13Gy puts the facial nerve at risk. There is evidence that the radiation dose to the cochlea affects whether hearing will ultimately be preserved. As such, if there is meaningful hearing at the time of treatment, the mean cochlear dose should be set to 4.2Gy or less. The cochlea is separately contoured at the time of treatment off fine cut T2 sequences which are then fused to the post contrast T1 images.
This patient: This patient had a moderate sized , symptomatic acoustic neuroma with serviceable hearing. Gamma Knife was recommended. A Gamma Knife treatment was performed by Dr. Michael Brisman. The radiation oncologist was Dr. Leester Wu. A treatment plan was made that was very conformal to the tumor. A prescription of 12.5Gy to the 50% isodose line was delivered. This plan involved a mean cochlear dose of 3.5Gy.
Planned Follow-up: Anticipated follow-up involves MRI’s and clinical examinations. Most likely, this patient has been cured of her acoustic neuroma.

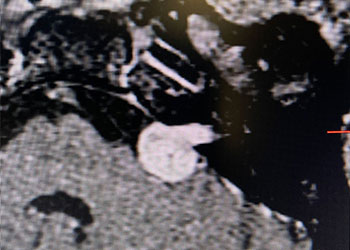
Image 1: Pre-operative imaging of the left acoustic neuroma.

Image 2: Intra-operative Gamma Knife treatment planning for the left acoustic neuroma. A tightly conformal treatment is set for 12.5Gy to the 50% isodose line. The cochlea has also been contoured, based off a fused image from a fine cut T2 sequence.

CATEGORY: BRAIN // ACOUSTIC NEUROMA
55 year old woman with one year of progressive hearing loss in the left ear / Acoustic Neuroma
This is a 55 year old woman with a history of hypertension who sought attention because of one year of progressive hearing loss in the left ear. The hearing in that ear was now about 50% of normal. She also had ringing in the left ear (tinnitus). She had no problems with her right ear. Her balance was normal and she had no other complaints. Formal audiology testing confirmed hearing loss in the left ear only. MRI with and without gadolinium demonstrated a 1.3 cm solid mass in the left cerebello-pontine angle and internal auditory canal that showed homogeneous enhancement, consistent with an acoustic neuroma.