- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
A Good Solution For Patients With Osteoporosis Who Need Surgery for a “Slipped Disc” or Spondylolisthesis
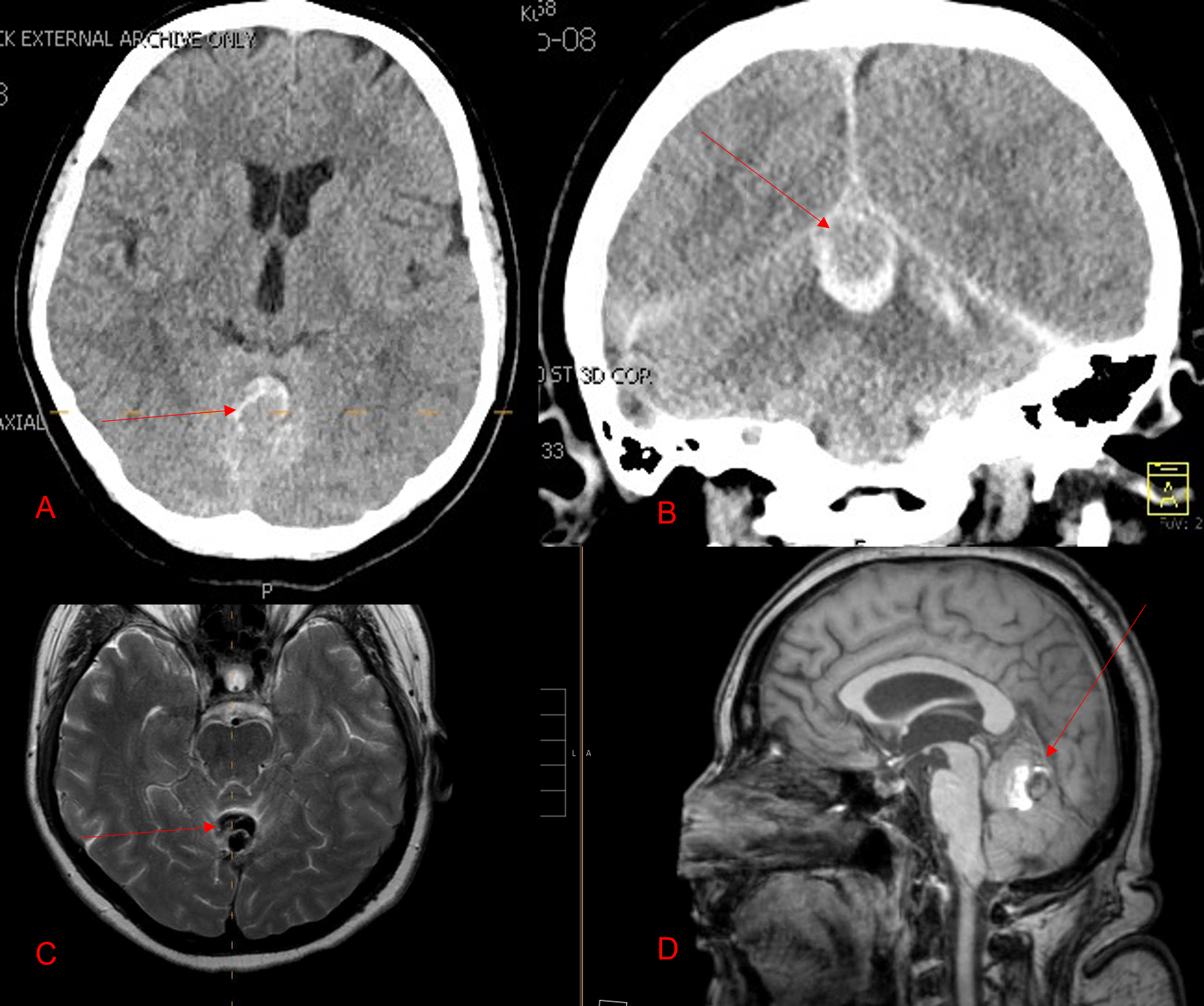
Ruptured Dural AV Fistula/AVM of the Posterior Fossa
August 29, 2022
A Good Solution For Patients With Osteoporosis Who Need Surgery For A “Slipped Disc” or Spondylolisthesis
July 26, 2023I specialize in and am very familiar with patients who have osteoporosis and require spinal surgery for degenerative lumbar disease. I am particularly interested in treating those osteoporotic patients with spinal stenosis and a concurrent spondylolisthesis or “slipped spine” or “slipped disc”. It is actually not the disc that slips in a spondylolisthesis, but one vertebra slips forward on the one below. As a result of this degenerative laxity the spine is signaled to make arthritis such as enlarged joints or thickened ligaments to compensate for the chronic instability that mainly contribute to narrowing of the spinal canal where the nerves travel. This is called spinal stenosis. Patients often see their MRI reports and note that they often have been described as having this aforementioned condition. I believe that perimenopausal, menopausal, and postmenopausal women (40-60 years of age) would benefit greatly because of their degree of activity and expectations from a new technology that my spine team is offering. However, this is not to say that men or women at any age who do require surgery would not benefit. A patient comes into the office and requires surgery to fix their slipped disc or spine and they say to me, “doctor but I have osteoporosis.” I tell them that we have available special coated screws that are designed for patients with osteoporosis that will do a much better job holding their bones together. Pedicle screws can be coated with a thin layer of hydroxyapatite (Fig 1)

(Fig 1) Hydroxyapatite Coated Pedicle Screw
This 59 year-old female had severe bilateral leg pain and numbness over a 6 month period. The patient had failed conservative treatment with physical therapy, chiropractic care, and medications. MRI revealed that she had severe lumbar stenosis with a grade 1 spondylolisthesis or “slipped disc” at L5-S1 (Fig 2).
In addition, she had previously undergone both front and back surgery for severe cervical stenosis where her posterior hardware had failed because of her severe osteoporosis requiring us to remove the posterior hardware . This required her to have an anterior or front operation which allowed better fixation to her spine because of the load-sharing nature of the interbody grafts in addition to her anterior cervical plate (Fig 3).

(Fig 3) Lateral Intraoperative Cervical X-ray demonstrating good alignment after C4-C6 anterior cervical discectomy and interbody fusion with plate. Note the interbody grafts help load share the plate in this patient with severe osteoporosis.