- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
Man in 40’s with progressive confusion and headaches
Carotid Cavernous Fistula (CCF)
October 27, 2021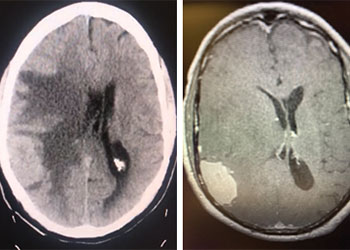
Atypical Convexity Meningioma
October 27, 2021
Educational Goals:
Learners will be able to recognize the symptoms that may suggest a symptomatic brain aneurysm, order appropriate tests to confirm the diagnosis, and appropriately refer these patients to a subspecialist for management and treatment.
A man in his 40’s experienced an acute onset of a moderate headache. Over the next 3 days, his family noticed increased lethargy, decreased appetite, and gait imbalance, which prompted them to bring him to the ED for evaluation. Initial CT scan of the brain confirmed diffuse subarachnoid hemorrhage with hydrocephalous, which required emergent EndoVentricular Drainage for a progressive diminished level of consciousness, WFNS Grade 3-4 (Figure 1).
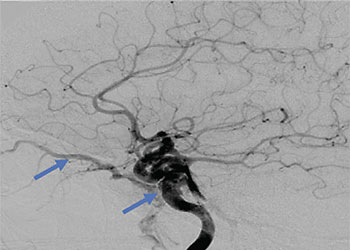
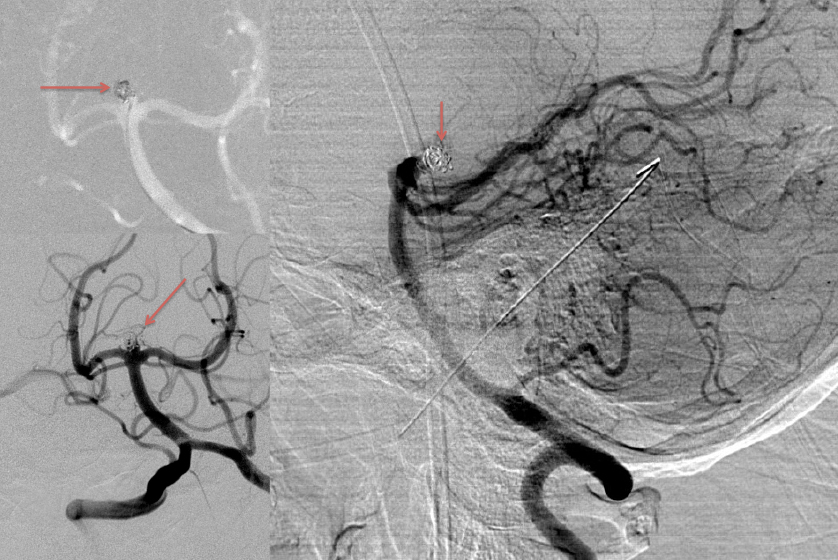
Urgent Cerebral Angiography confirmed a 5 mm posteriorly projecting aneurysm of the Basilar Artery Apex (Figure 2 A, B). Based on the location, morphology, and posterior projection, we decided to proceed to coil embolization of this high-risk aneurysm to prevent catastrophic re-bleeding and afford us the opportunity to maximize critical care for this patient during his hospital course. In this aneurysm, the dome-neck ratio was favorable from primary coiling, which was successfully performed resulting in near-complete embolization of the aneurysm (Figure 3 A, B). After 2 weeks of continued critical current l, endovascular, and neurosurgical care for complications of subarachnoid hemorrhage, including vasospasm and hydrocephalous, he was able to make a complete recovery and ultimately discharged home to complete his recovery, having regained all neurologic functions and activities of independent daily living and planning a return to work as an executive professional in the near future.
Figure 1: Non-Contrast CT of the Brain demonstrates diffuse subarachnoid hemorrhage(red) and early dilatation of the temporal horns consistent with hydrocephalous (yellow).
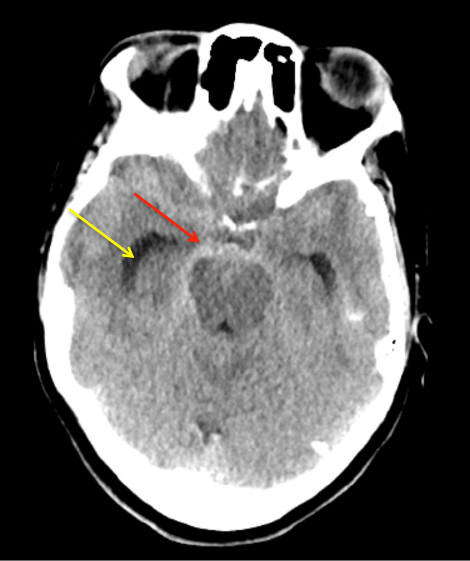
Figure 2: A) AP DSA angiogram demonstrates a 5 mm posteriorly projecting aneurysm of the Basilar Apex B) 3D DSA confirms the morphology and favorable dome to neck ratio for primary coil embolization.
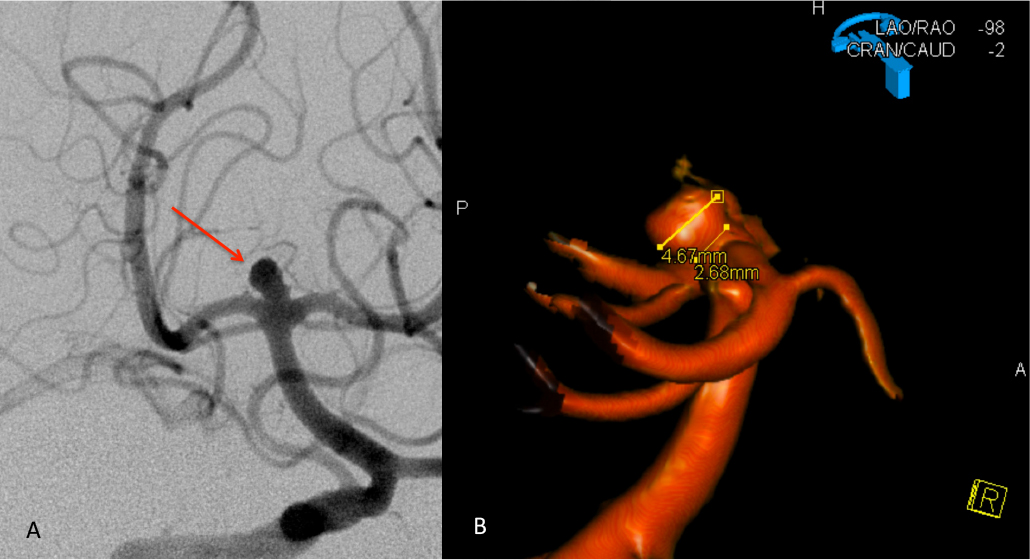
Figure 3: A) Initial Coil placement in Aneurysm dome B) Final AP and C) Lateral DSA demonstrating near complete obliteration of the ruptured aneurysm
Discussion:
Clinical presentations for rupture of a brain aneurysm are often diverse and may be difficult to determine. Classically, patients experience “the worst headache of their life” (WHOL), that may persist despite pain medications and may progress to lethargy, confusion, focal neurologic deficit, or coma. Initial symptoms may often be over-looked by the patient, and require a detailed examination from the medical team, including CT scan and Lumbar Puncture to identify life-threatening subarachnoid hemorrhage. A screening CT of the brain is often the initial study that raises the index of suspicion, augmented by a detailed clinical history and physical examination of the patient.
The natural history of untreated ruptured aneurysms remains poor with studies suggesting re-bleed rates from 1-4% daily, and mortality rates approaching 50-60% at 1 year. Early multi-disciplinary management of medical risk factors such as hypertension and hydrocephalous, as well as securing the brain aneurysm from re-bleeding events is critical to enhanced functional survival. The choice of treatment has evolved over the last several decades, with traditional microsurgical clipping now complemented with less invasive neuroendovascular techniques such as primary coil embolization as applied in this patient. Our experiences over the last 20-30 years with Neurointerventional Techniques have demonstrated high levels of safety, efficacy, and durability, in both posterior and anterior circulation brain aneurysm patients. The prognosis of ruptured aneurysms, when treated successfully and when presenting with milder grades (WFNS 1-3) are often favorable with high levels of functional recovery defined as a Modified Rankin Scale of 0 to 2. Even higher-grade patients can often experience a highly functional recovery, especially when treated early by an experienced multi-disciplinary team (References 1-3).
References:
- Lusseveld, E., Brilstra, E. H., Nijssen, P. C., van Rooij, W. J., Sluzewski, M., Tulleken, C. A., Wijnalda, D., Schellens, R. L., van der Graaf, Y., & Rinkel, G. J. (2002). Endovascular coiling versus neurosurgical clipping in patients with a ruptured basilar tip aneurysm. Journal of neurology, neurosurgery, and psychiatry, 73(5), 591–593. https://doi.org/10.1136/jnnp.73.5.591
- Korja, M., Kivisaari, R., Rezai Jahromi, B., & Lehto, H. (2017). Natural History of Ruptured but Untreated Intracranial Aneurysms. Stroke, 48(4), 1081–1084. https://doi.org/10.1161/STROKEAHA.116.015933
- Molyneux, A. J., Birks, J., Clarke, A., Sneade, M., & Kerr, R. S. (2015). The durability of endovascular coiling versus neurosurgical clipping of ruptured cerebral aneurysms: 18-year follow-up of the UK cohort of the International Subarachnoid Aneurysm Trial (ISAT). Lancet (London, England), 385(9969), 691–697. https://doi.org/10.1016/S0140-6736(14)60975-2
Disclosures:
The planners and faculty participants do not have any financial arrangements or affiliations with any commercial entities whose products, research or services may be discussed in these materials.
CME Accreditation:
This activity has been planned and implemented in accordance with the accreditation requirements and Policies of the Medical Society of the State of New York (MSSNY) through the joint providership of the Academy of Medicine of Queens County and NSPC Brain and Spine Surgery. The Academy of Medicine of Queens County is accredited by The Medical Society of the State of New York (MSSNY) to provide continuing medical education for physicians. The Academy of Medicine of Queens County designates this Enduring Materials for a maximum of .5 AMA PRA Category 1 Credits™ as specified in this activity. Physicians should claim only the credit commensurate with the extent of their participation in the activity.