- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
Severe Intractable Postural Headaches in a Young Lady

Patient with Cervical Spine Trauma Suffers Multiple Concurrent Pathologies
March 26, 2022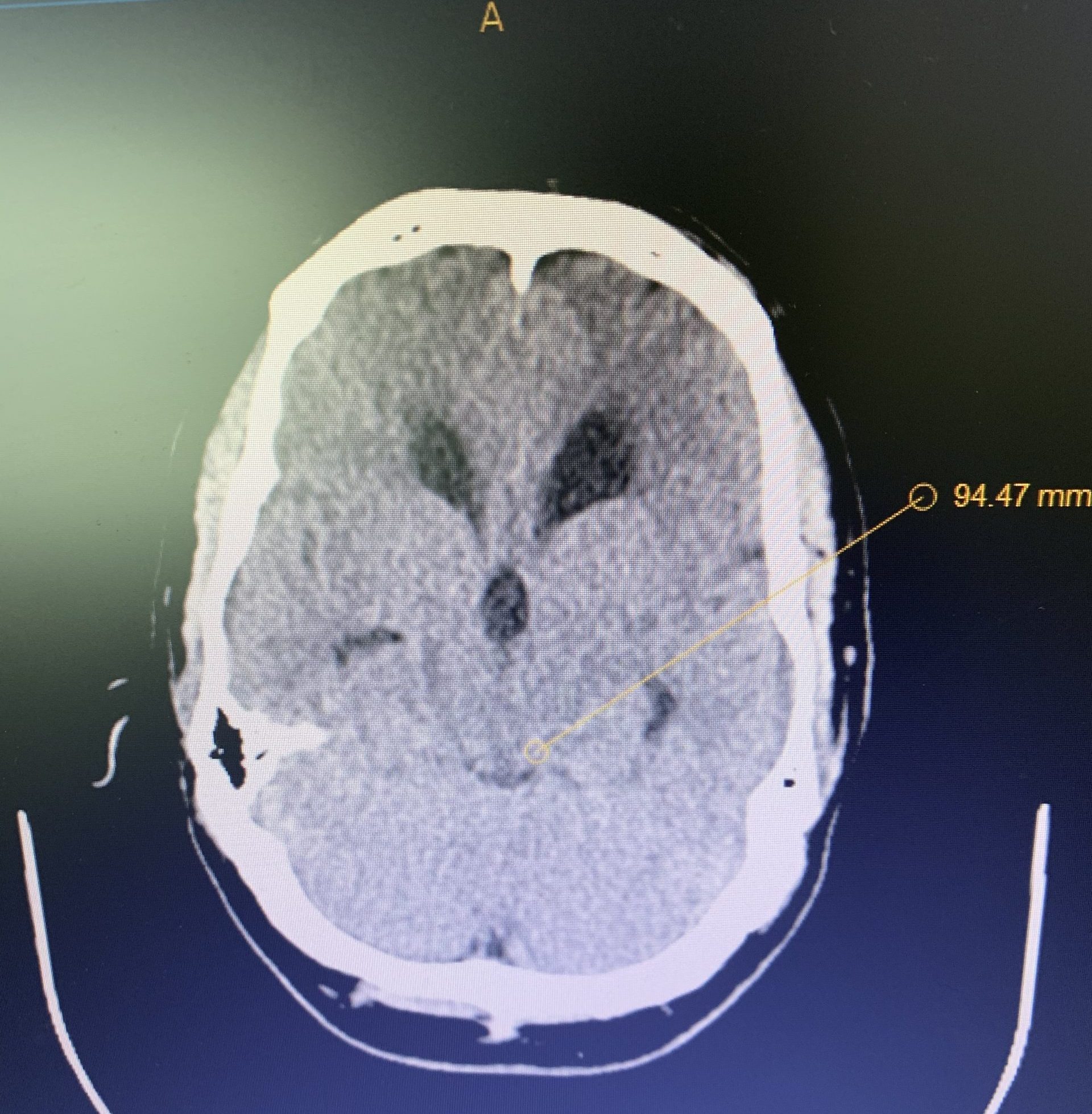
Hydrocephalus and Brainstem Tumor
April 8, 2022A young lady presented with a myriad of disabling difficulties, after a flourishing adolescence full of academic and athletic successes.
Her headaches, located on the top of her head, radiating to the neck and behind her eyes, were worse in the evening and made worse by standing. She had joint hypermobility (“double jointed”). Episodes of palpitations, postural orthostatic tachycardia, (POTS), and dysautonomia, severe nausea, difficulty swallowing, syncope, phonophobia, photophobia, and diplopia plagued this resilient soul.plagued this resilient soul. Despite this, she continued to work.
Imaging and other provocative diagnostic test showed the associated problems of Cranial Cervical Instability, incidental thoracic syringomyelia, Hashimoto Thyroidistis, Polycystic Ovarian Syndrome, Nutcracker Syndrome, Postural Orthostatic Hypotension, and Hypo/Hyper intracranial Pressure with spontaneous CSF leaks.
A formal diagnosis of Ehlers-Danlos Syndrome (EDS), a connective tissue disease, was made. There are 13 recognized types of this condition, both autosomal dominate and recessive. There is a broad range of presentations. Many, as in her case, are associated with many difficulties. Treatment is symptomatic and protracted.
Thankfully, marked improvement of her brainstem and lower cranial nerve function, demonstrated on trial cervical traction improved with Cranial-Cervical Fusion.
Her symptoms of Intracranial hypotension have been challenging.
Imaging.
As in her case, MRI imaging, with heavily weighted T2 Fat-Saturated Sequences (3D-T2WI-FS) provide a very high accuracy for the CSF leak presence into the epidural space. Multiple imaging sites are usually identified, although at surgery or with dynamic CT myelography, only one site is found.
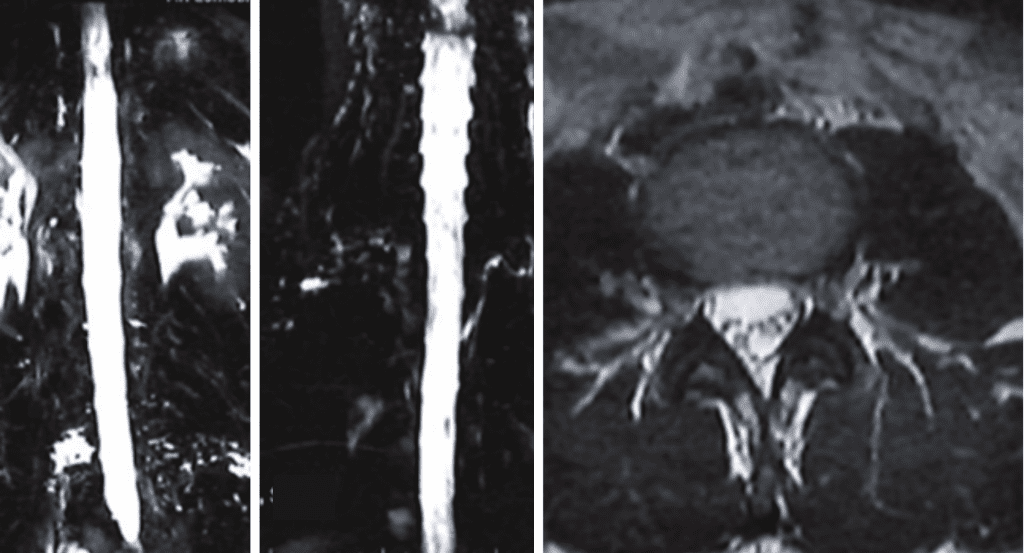
Fig 1. MRI myelogram with fat saturation showing multiple fluid areas along nerve root areas in the high and low lumbar region, consistent with CSF leaks.
Etiology.
The thin Dura in patients with EDS can dehisce at any point. Other causes include on osteodiscophyte penetrating the Dura, or rupture of a spinal nerve root diverticulum. Recent appreciation of other mechanism of Spontaneous Intracranial Hypertension (SID) includes CSF-Venous Fistula.
Blood Patching.
High Volume Blood patches under X-ray guidance, with a very small needle, being careful not to puncture the dura is indicated. This usually give relief lasting days to months. It may well need to be repeated.
Fibrin Patching.
Injection of fibrin glue into the epidural space, has a much greater chance of healing the CSF leaks. However, it can also impair “normal” CSF dynamics in these abnormally compensated situations, leading to intracranial hypertension.
Spontaneous Intracranial Hypotension (SIH) associated with EDS is often a complex disease. I am thankful to be part of a strong team that can address the plethora of problems these patients face.
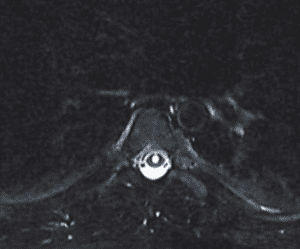
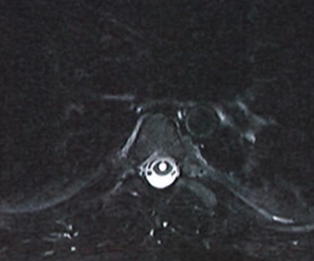
Fig 2. MRI of thoracic spine showing syringomyelia.
CATEGORY: ENDOVASCULAR // SEVERE INTRACTABLE POSTURAL HEADACHES IN A YOUNG LADY
Severe Intractable Postural Headaches in a Young Lady