- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
Hydrocephalus and Brainstem Tumor
Severe Intractable Postural Headaches in a Young Lady
April 1, 2022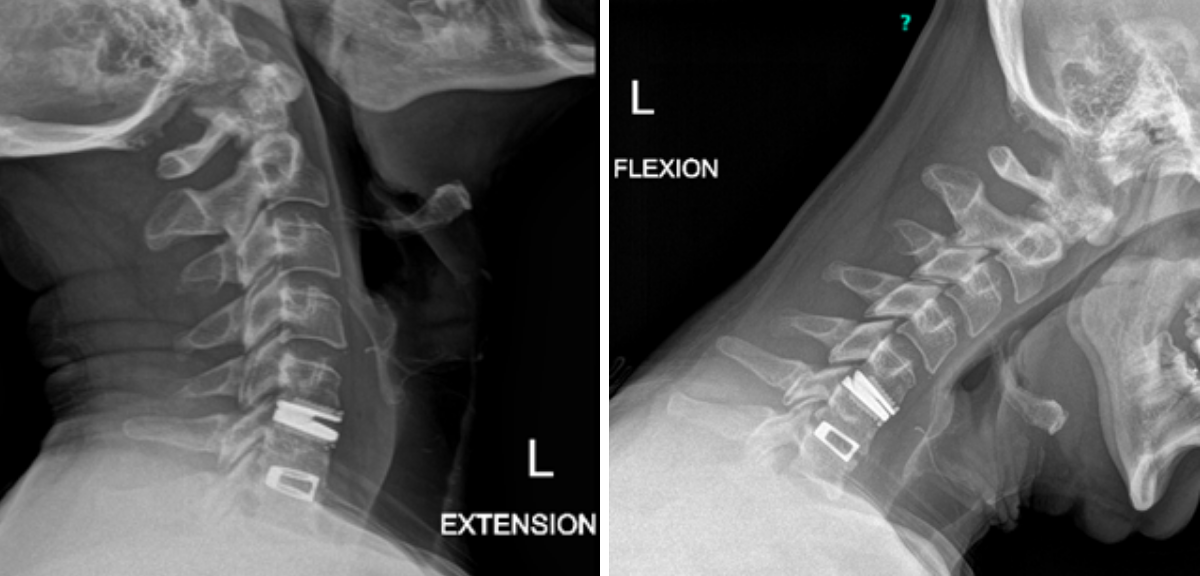
Non-Fusion Alternative for Treating Adjacent Segment Disease
April 14, 2022The patient is a 59-year-old gentleman who is otherwise healthy, but states that he had a traumatic head injury several months prior for which he was hospitalized and had some intracranial bleeding.
He presented several months later to a neurologist in order to get a driving clearance and an MRI was performed showing hydrocephalus.
On initial examination, the patient was neurologically intact without complaints of headache. His imaging; however, did show hydrocephalus, most notably the lateral and third ventricles with a normal sized fourth ventricle. Given that the patient had no complaints, a decision was made to follow this expectantly and he was referred for a neuro-ophthalmologic evaluation, which confirmed no evidence of papilledema. MRI was otherwise negative.
Several weeks later, the patient re-presented to the office complaining of significant headaches and gait disturbance and a decision was made at that point to recommend shunting.
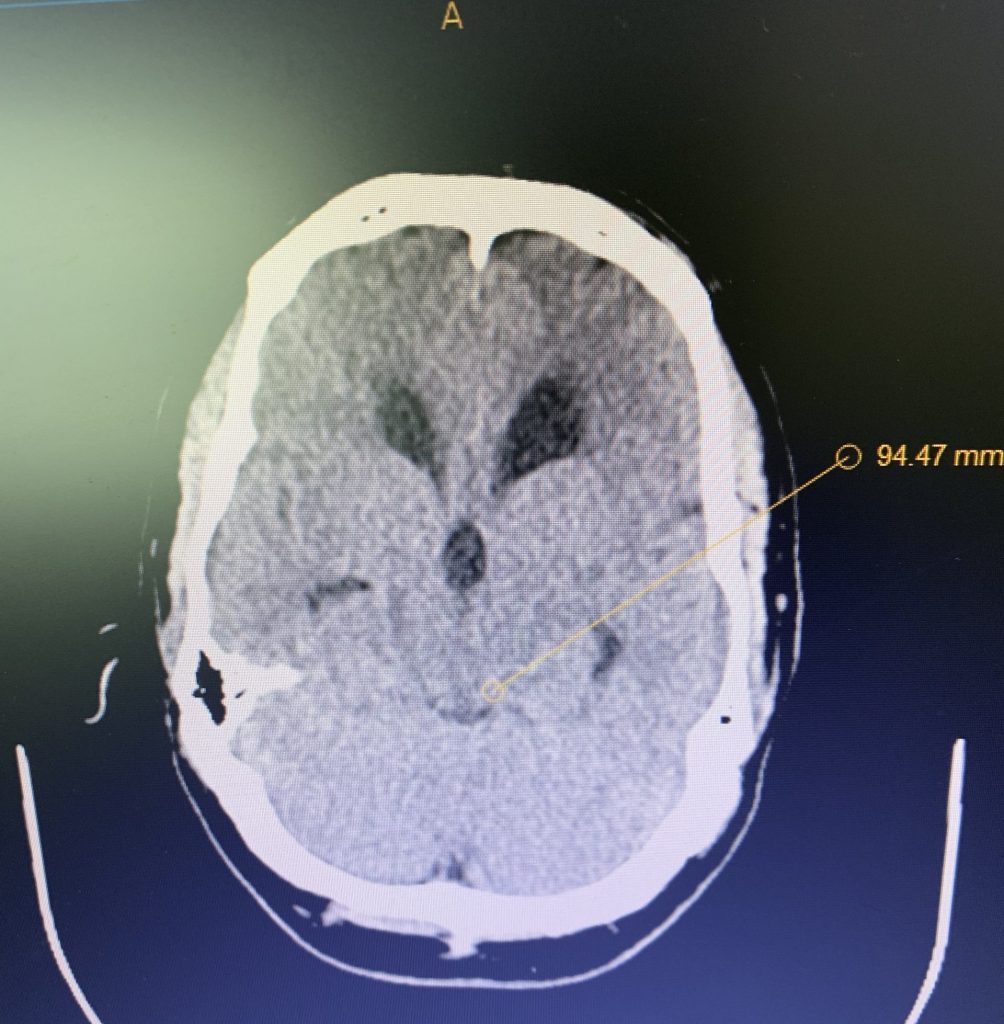
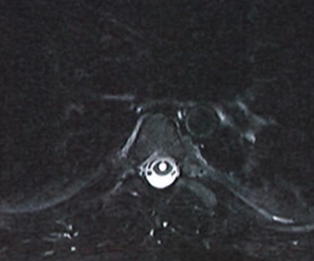
Figure 1A: Pre-operative MRI
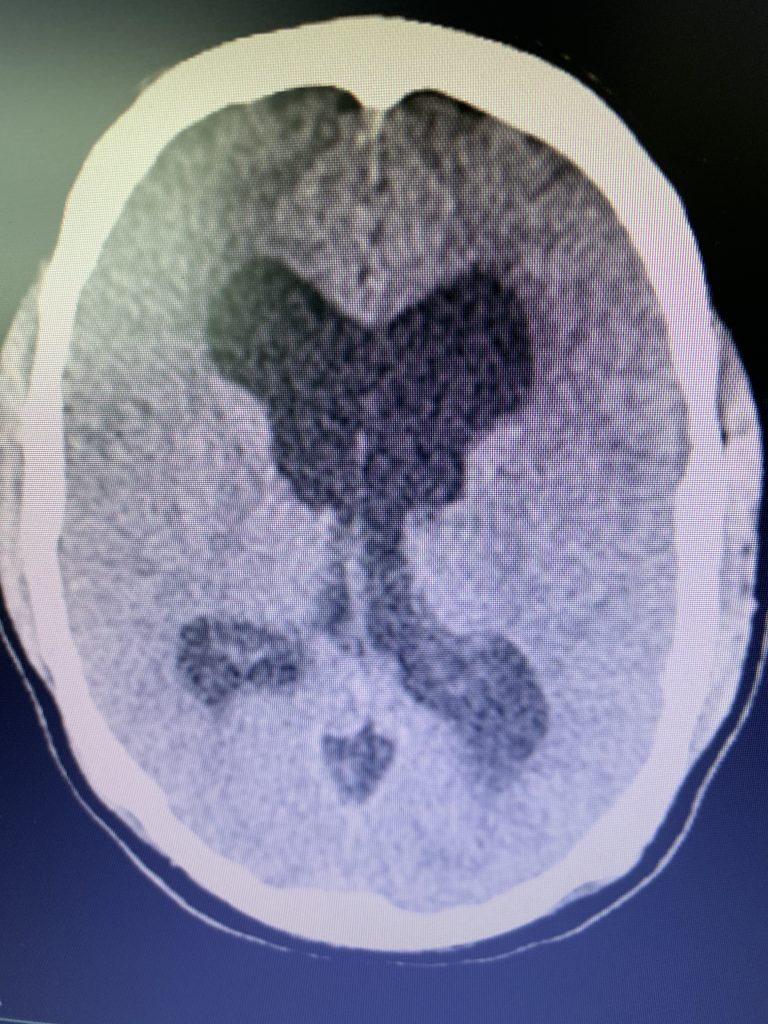
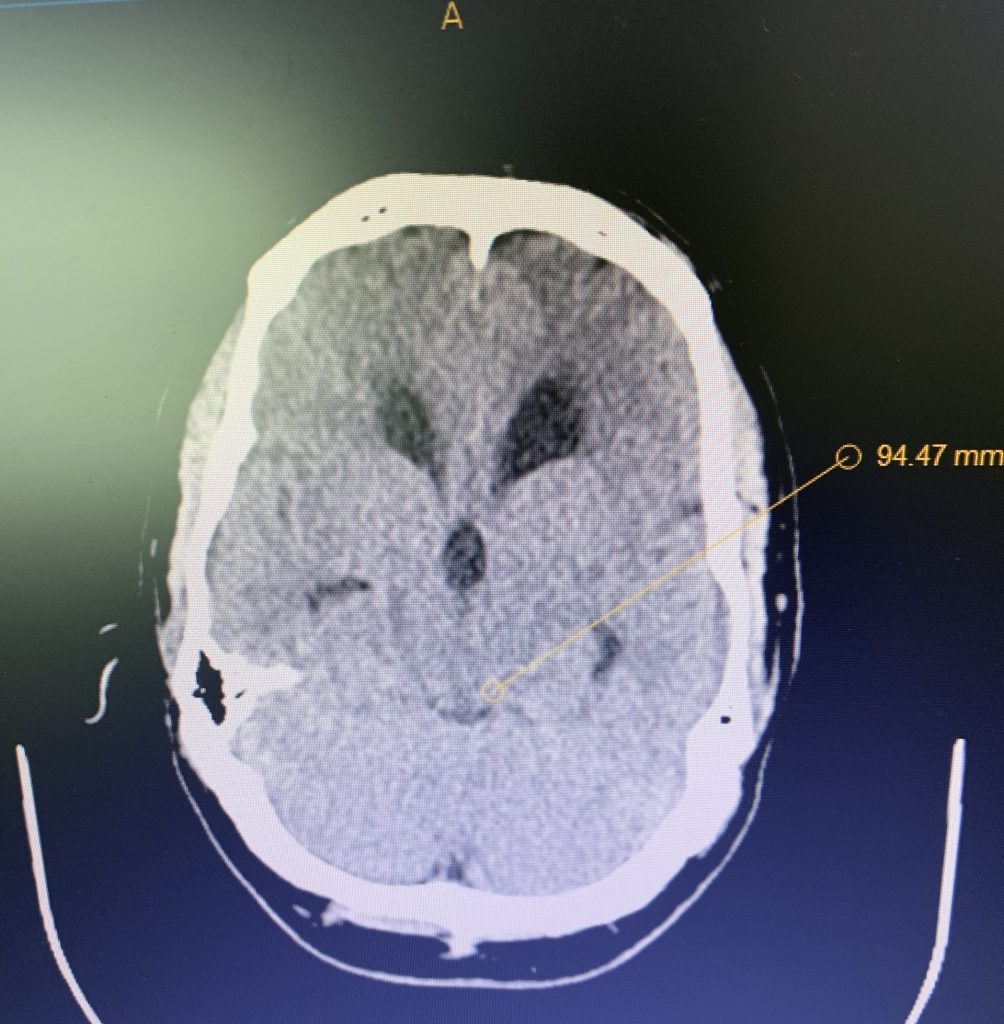
Figure 1B,C: Pre-operative CT images.
Prior to shunting, a head CT was obtained and the head CT in addition to documenting a patten of obstructive hydrocephalus suggested a possible mass lesion compressing the aqueduct at its inferior aspect. Figure #1 demonstrates the hydrocephalus and the possible lesion. A decision was made at this point that the patient had obstructive hydrocephalus that was now symptomatic and he was taken for a laparoscopic-assisted ventriculoperitoneal shunt.
I placed a Strata valve, which is a percutaneously programmable valve set at 1.5, which is essentially a medium pressure. I implanted that and then tunneled it into the abdomen with the assistance of a general surgeon such that the procedure was performed laparoscopically without significant incisions on the abdomen.
The patient was discharged the following day and has noted marked improvement in his headaches and no longer feels unsteady when working.
QUESTIONS AND ANSWERS:
Question 1: What is the differential diagnosis for this tumor and what is his prognosis and treatment strategy?
Answer: This is most likely a benign intraaxial low-grade glioma. These tend to be indolent. He will be followed up with serial MRIs with gadolinium and unless there is a growth or otherwise change in the lesion, this will be followed expectantly.
Question 2: Was there a role for any additional workup on the initial presentation such as a spinal tap?
Answer: No, in fact, given the normal fourth ventricular size, the patient most likely has obstructive hydrocephalus and a spinal tap could prove disastrous as it could encourage brain herniation via reduction in intracanal pressure in the spinal region.
Question 3: What was the particular pitfall in this case?
Answer: The patient gave a history of traumatic intracranial hemorrhage, which can lead to hydrocephalus. The patient was unable to supply those images and, therefore, we were working under the presumption that this was hydrocephalus secondary to trauma and hemorrhage when, in fact, the lesion was not well visualized on the initial MRI due to patient motion.
Question 4: Was endoscopic third ventriculostomy considered for this patient?
Answer: Endoscopic third ventriculostomy would be a consideration, as it is in most cases of obstructive hydrocephalus. My experience, however, has been that it is not as definitive as shunting and given concerns over noncompliance with this patient, I felt that that a potentially curative shunt was the best treatment strategy.
CATEGORY: ENDOVASCULAR // HYDROCEPHALUS AND BRAINSTEM TUMOR
Hydrocephalus and Brainstem Tumor