- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
LUMBAR SURGERY CAN BE DONE IN THE MORBIDLY OBESE PATIENT

When Just Enough is Enough
January 11, 2024
NSPC Spring 2024 Spine Newsletter
March 18, 2024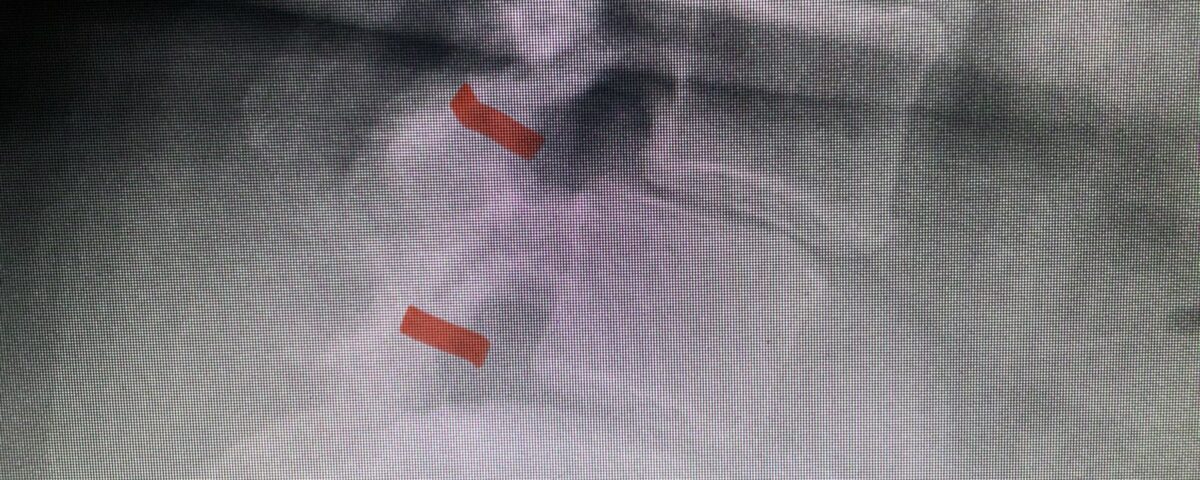
As a spine surgeon you see patients with all body types. Morbidly obese patients pose a particular challenge. Heavy patients who have lumbar spinal stenosis or a herniated disc and a slipped or misaligned vertebrae sometimes will require surgery. One particular challenge intraoperatively is the depth of exposure and the limitation of the length of the instruments. One positive is that these patients often do not have a great deal of muscle mass which makes it easier to retract the tissues in order to gain exposure.
As a spine surgeon, patient selection is critical for a successful surgical outcome. Even an obese patient, if they have spinal stenosis and symptoms that correlate with their imaging studies, have very successful outcomes and relief of leg pain just as much as a thin person. Back pain is a little more mysterious because of extra weight and strains that are independent of what was done surgically and may be more difficult to solve until the patient actually loses weight. I am happy to see you no matter what your weight is, especially if you have been told you can’t have surgery because of your weight as a second opinion.
If you are reading your radiology reports, you will notice that you may have a grade 1 spondylolisthesis at L4-5 with moderate or severe stenosis. You may have a herniated disc. You may also have had spinal surgery ten or fifteen years ago and now have new problems with pain down your legs and a new area above your prior fusion with new stenosis and perhaps an associated spondylolisthesis as well. Patients who are obese and have symptoms of spinal stenosis or herniated disc such as pain down their legs when they walk cannot exercise. They become depressed because of weight gain and eat more and hence a vicious cycle develops. Exercise really makes people feel good and therefore these patients are not experiencing these beneficial feelings. The pain from spinal stenosis or herniated disc and/or slipped vertebrae or spondylolisthesis (in Greek: slipped spine) can be disabling, particularly the pain down the legs.
It is well studied and an accepted community standard that a patient with spinal stenosis or herniated disc and concurrent spondylolisthesis who has failed conservative management and undergoes surgery should not only have a laminectomy for decompression for their lumbar stenosis, but also should have a concomitant fusion with or without instrumentation. What is a fusion? People are more frightened about this part of the procedure than the laminectomy itself which is really the part of the procedure that is most challenging in my opinion. Fusion just means to connect two spinal segments with usually a combination of bone dust and titanium screws which are indeed MRI compatible. This is not a nuclear fusion! What the fusion simply accomplishes is to stabilize the segment preventing abnormal motion. This does in fact improve not only clinical outcome but will also arrest the signal to make more arthritis and hence prevent recurrent stenosis.
It is essential post operatively to mobilize to prevent DVT and pneumonia and infection especially if the patient is diabetic. Because of the degree of dead space created during the surgery, these patients can develop wound collections or seromas and because of their lack of mobility, often develop wound drainage issues. I find it useful to enlist the aid of a plastic surgeon in wound closure and post operative care. Here are some case studies of morbidly obese patients with very reasonable arguments for surgery, despite their weight:
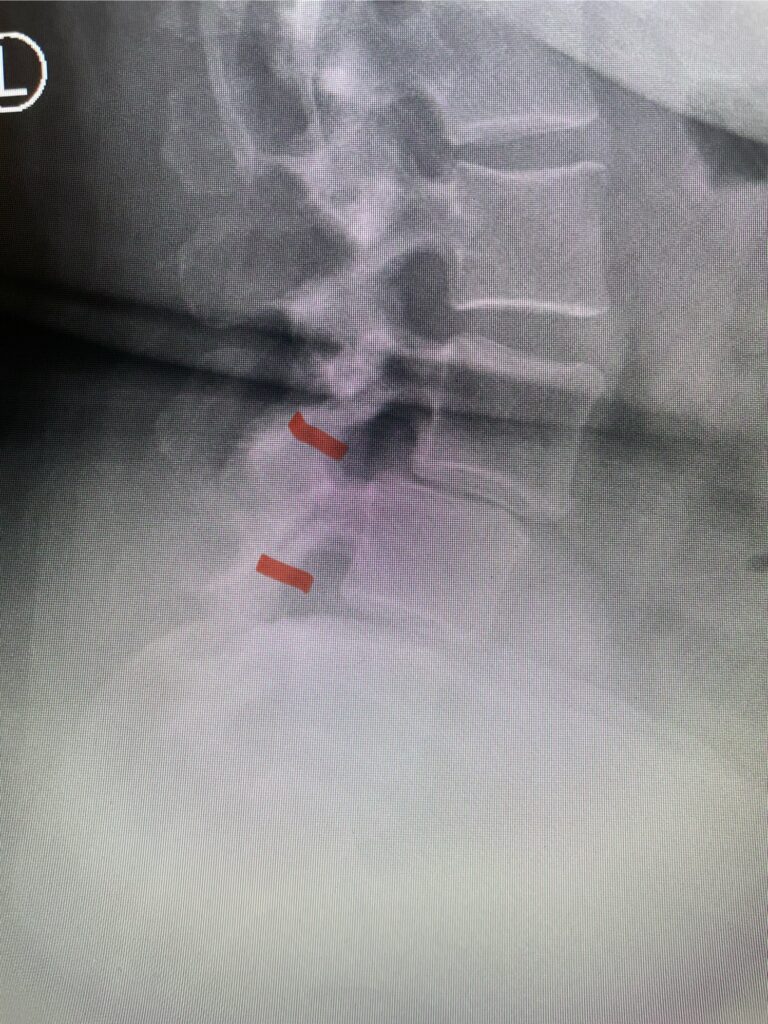
This 54-year-old morbidly obese female presents with progressive back and leg pain and quadriceps weakness. She had no diabetes. She failed all means of conservative management including physical therapy and epidural injections. On imaging she had severe stenosis at L3-4 with a disc protrusion and a slight grade 1 spondylolisthesis at L3-4 (Fig 1). We performed dynamic lumbar x-rays which demonstrated instability at L3-4 and L4-5 (Fig 2). The patient wished to have surgery. We performed an L2-4 decompressive laminectomy and L3-5 in situ fusion because of her instability. Post operatively the patient had relief of leg pain, although the patient was slow to mobilize.

Figs. 1a: Sagittal lumbar T2-weighted MRI demonstrating severe lumbar stenosis with a slight grade 1 at L3-4 and a disc protrusion (red arrow )

Fig 1b: Axial lumbar T2-weighted MRI demonstrating severe lumbar stenosis (red dot)
")
Fig 2: Lateral preoperative lumbar x-ray demonstrating L3-4 and L4-5 spondylolisthesis on flexion.
The next patient is a 56-year-old morbidly obese female who had progressive leg pain and weakness. She was over 320 lbs and did not have diabetes either. On MRI she had a massive disc herniation spanning the L3-4 and L-4 interspaces, centered behind the L4 vertebral body (Fig 3A and B). She also had an L4-5 spondylolisthesis. There were opinions that the disc emanated from the L3-4 disc space, but because of spondylolisthesis and on careful inspection of the MRI, there was a high chance the disc herniation had instead emanated from L4-5 (Fig 4). She had conservative treatment including epidurals but had worsening strength and numbness. She was scheduled electively for surgery, but then fell, and broke her ankle. She could not walk, particularly due to the pain down her leg. She was taken to the operating room urgently after she was cleared medically. She had no issues cardiologically and was taken to the operating room. The patient underwent a laminectomy that extended above the L3-4 disc space to below the L4-5 disc space. We encountered mainly centered on the left at the level of the L4 vertebral body and massive disc herniation that created a huge cavity in the lumbar canal. It was covered in an interesting thin membrane that we dissected off the disc herniation (Fig 5). Postoperatively the patient did experience significant relief of pain, but some improvement of strength. In combination with the ankle fracture and the extent of preoperative weakness, the patient required extensive rehab. The patient also developed a seroma and some wound drainage issues that were treated locally.

Fig. 3a : Sagittal T2-weighted lumbar MRI demonstrating a massive L4-5 disc herniation with superior migration behind the L4 vertebral body and taking up most of the left side of the spinal canal (red arrow) Note the slight grade one spondylothesis at L4-5 (blue dash). Notice the severe compression of the thecal sac (blue arrow) by the large left sided disc herniation (red arrow)

Fig. 3b: Axial T2-weighted lumbar MRI demonstrating severe compression of the thecal sac (blue arrow) by the large left sided disc herniation (red arrow) taking up most of the left side of the spinal canal (red arrow)

Fig 4: Sagittal T2-weighted lumbar MRI demonstrating an L4-5 grade 1 spondylolisthesis with obvious emanation of the disc herniation from the L4-5 level (red arrow)

Fig 5: intraoperative photo demonstrating the massive size of the L4-5 disc after removed.