- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
NSPC Mobile Patient
Grade 1 Spondylolisthesis At L4-5 With Severe Lumbar Stenosis
May 9, 2022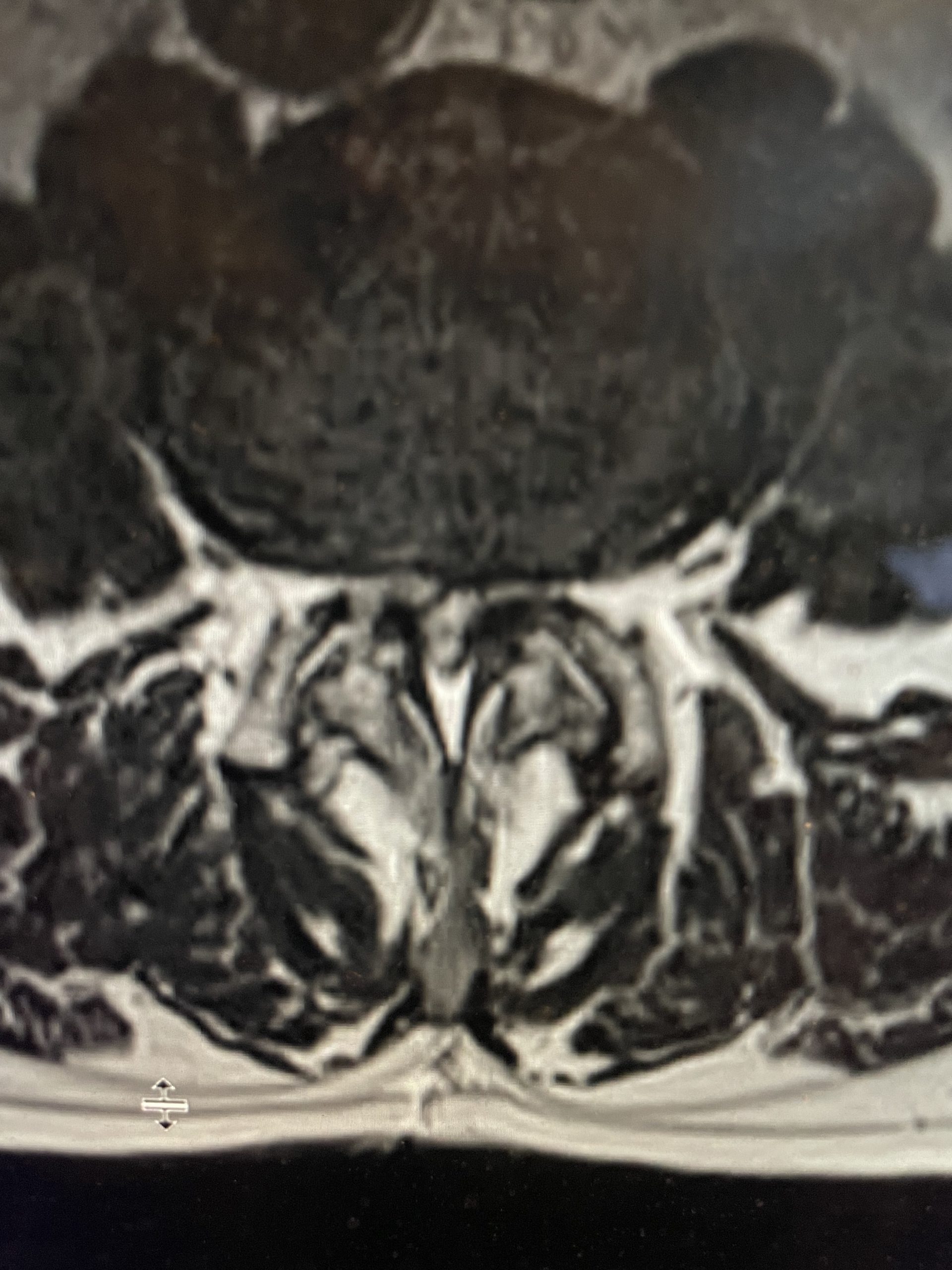
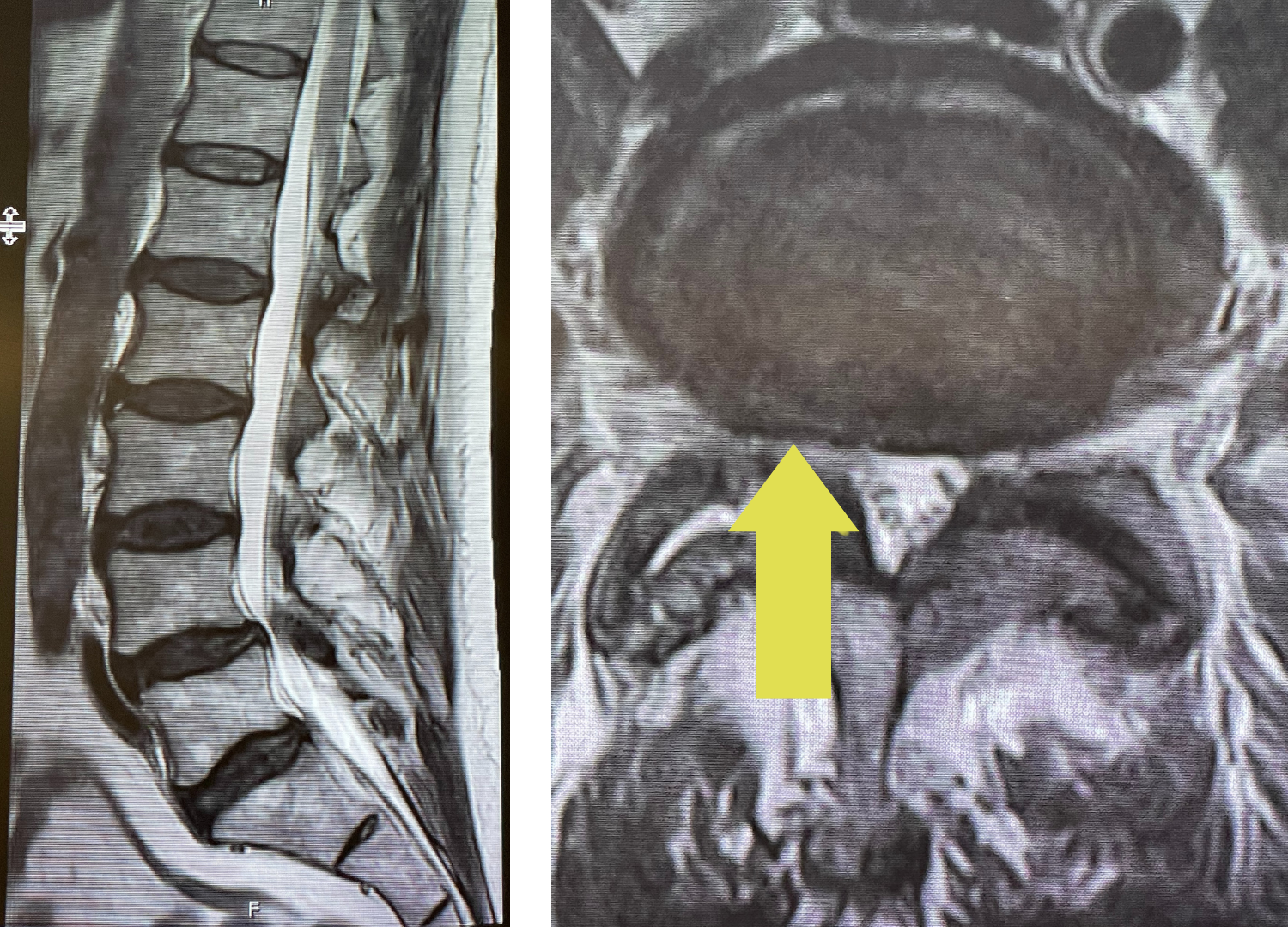
Severe Stenosis With A Grade 1 Spondylolisthesis
May 11, 2022
IMG 5090 768x1024 1

Figure 1: Sagittal x-ray after C6-7 anterior cervical discectomy showing collapse of the C5-6 disc space with fully connected anterior bridging osteophyte and C4-5 partially bridged anterior osteophyte with anterior angulation of C4 vertebral body. Sagittal T2-weighted MRI showing listhesis of C4 on C5 with C4-5 disc protrusion causing cord compression.
Another patient followed up who I initially had seen on our NSPC mobile van at her worksite. She was 52 years-old and complained of chronic intractable left greater than right arm pain and tingling. She had had a prior anterior cervical discectomy and fusion with plate at C6-7 by another surgeon.
On the initial visit she was completely neurologically intact. We recommended physical therapy and ordered cervical x-rays and MRI (Fig 1). It appeared on her x-rays that she had a stable C6-7 fusion segment, but she also had a very collapsed C5-6-disc space. In front of that C5-6 disc space there is an obvious anterior osteophyte bridging the space, in essence autofusing that segment. Right above that at the C4-5 space there was an anterior bridging osteophyte as well with some C4 anterior angulation and listhesis with respect to C5, although the bridging bone did not completely bridge across to C5. Since C6-C7 and C5-6 were essentially non functional, there was biomechanical stress on the next segment, C4-5, which resulted in premature degeneration and instability. This also on MRI caused more stress on the C4-5 disc segment and secondary protrusion with anterior cord distortion. Given this was only a static picture of her spine, imagine how her cord is affected on flexion and extension movements.
When she followed up this week she was noted to now have weakness in her left finger extensor muscles. She still suffered with neck, left shoulder, and arm pain and numbness despite the course of physical therapy. This illustrates why it is so important to follow these patients closely as she had a subtle change in her exam which reflected the findings on the MRI. We discussed the findings with the patient. We discussed various options, including pain management with an epidural and possibly surgery. If she had surgery to decompress the spinal cord by performing an anterior cervical discectomy and fusion at C4-5, we would need to include C5-6. In this case you would change the biomechanics because C5-6 is autofused. If it was not, then that is an issue particularly if the level in between is normal and floating between two fused segments. If that was the case and you fused the C4-5 segment then the C5-6 segment would be under a great deal of stress and possibly herniate. This is a tough situation because you don’t want to remove a normal disc. This is a controversial topic in spine surgery. The patient elected to try injections by pain management. She will be followed up in 6-8 weeks.

