- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
55 year old woman with balance problems and a large left frontal mass / Cystic Meningioma

74 Year Old Woman with Occipital Headaches
October 27, 2021
Fusionless Cervical Spine Surgery for Herniated Disc
October 27, 2021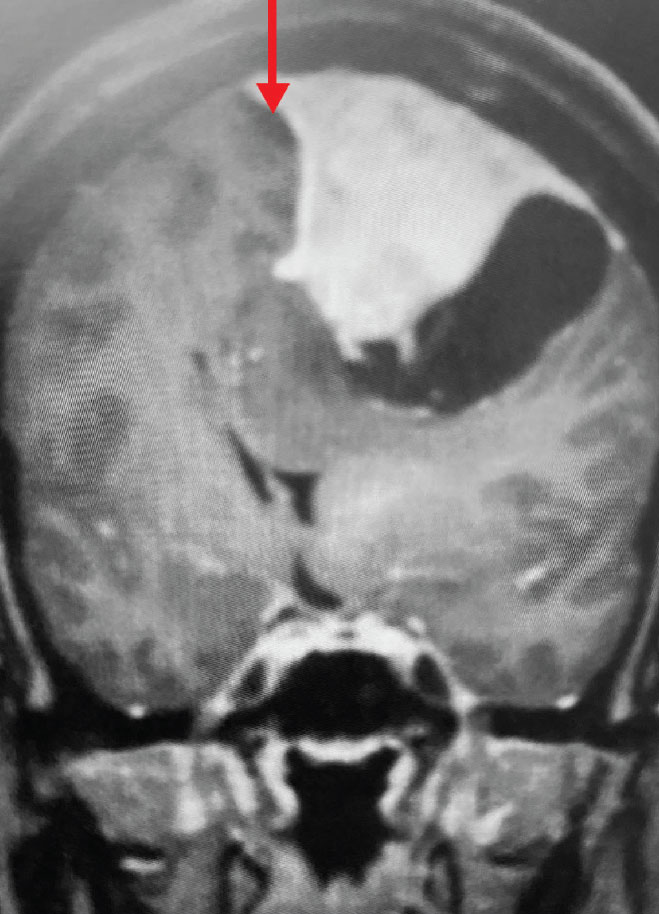
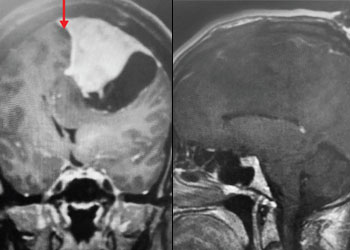
Fig 1. A) Pre-operative, post-contrast, coronal MRI. Arrow points to tumor involvement in the superior sagittal sinus.
Cystic Meningiomas: Sometimes meningiomas can have partly cystic (fluid) components. This does not necessarily mean the tumor will be of a higher grade, or behave differently than entirely solid meningiomas.
Convexity and Falx Meningiomas: While meningiomas can involve either the convexity or the falx alone, it is possible for such tumors to involve both structures. In this case, vascular supply to the tumor can originate from both dural sources. When meningiomas involve the convexity dura, the dura is often excised and replaced with a duraplasty (an artificial dural replacement). When tumors involve the falx, the falx itself is usually not removed in entirety.
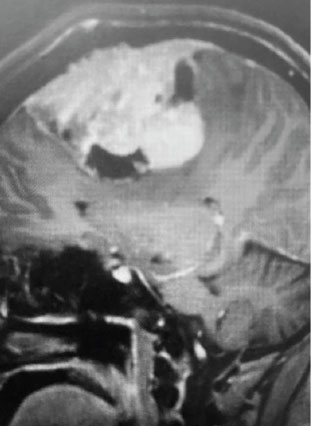
Fig 1. B) Pre-operative, sagittal post-contrast MRI.
Meningiomas that compress the motor strip: This meningioma was clearly compressing the left motor strip significantly, likely explaining the patient’s balance problems. That having been said, these tumors often have very distinct borders with the normal brain, and can be removed without harming the underlying motor strip.
Meningiomas of the dominant hemisphere: Meningiomas of the dominant hemisphere, usually the left hemisphere, can cause problems with language or “aphasias”. This patient did not have any language problems. Again, these tumors are usually very distinct from the surrounding brain, and can usually be removed without injuring the underlying brain tissues, such as those important for language processing.
Meningiomas that involve the superior sagittal sinus: Sometimes convexity or falx meningiomas will grow into the superior sagittal sinus. Sometimes the sinus can become completely occluded. Usually this occurs over many years, and as such, the brain has time to develop venous collaterals. So, while in a normal person, sudden occlusion of the superior sagittal sinus could lead to venous infarction or death, the very gradual occlusion that can be seen with meningiomas, does not lead to these problems. Also, if the sinus is filled with tumor and completely occluded, it can usually be safely removed at that segment.
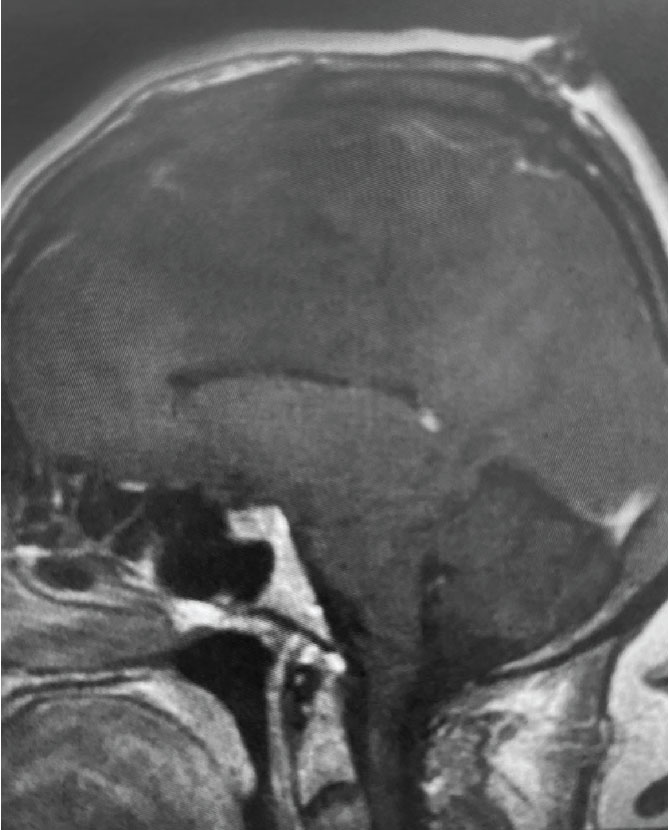
Fig 2. A) Post-operative, post-contrast, sagittal MRI.
Treatment: Given the size and location of this tumor, the best treatment was surgical removal. Surgery was performed by Dr. Michael Brisman. A craniotomy exposed the tumor along the convexity as well as the superior sagittal sinus. The tumor was removed, as was the involved convexity dura and the affected segment of the sagittal sinus. Removed dura and skull were replaced with duraplasty (with artificial dura) and a titanium mesh cranioplasty.
Outcome: The patient did very well and made a full recovery.
Summary: Meningiomas, even when very large, are usually benign tumors. In cases of large meningiomas, surgical removal can lead to dramatic improvement in symptoms and can be curative.
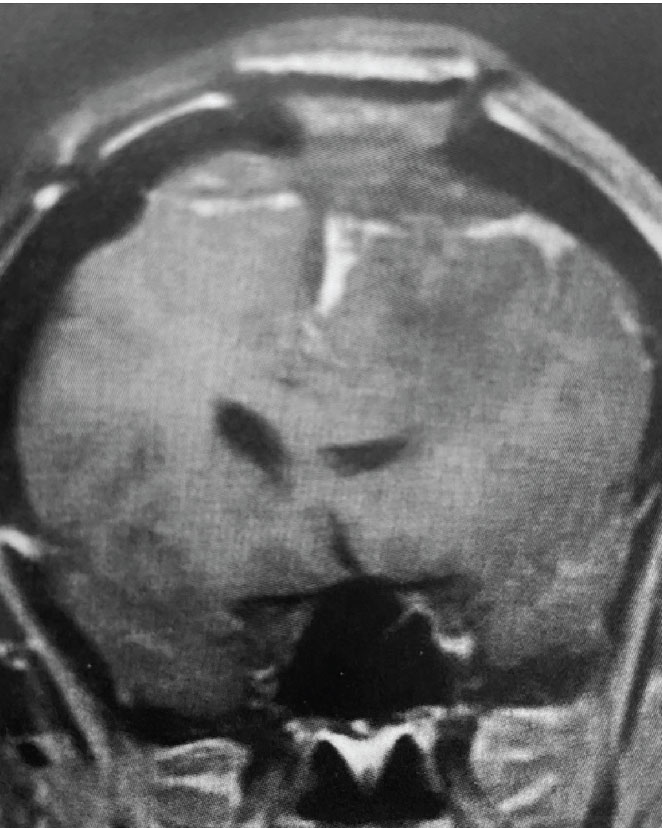
Fig 2. B) Post-operative, post-contrast, coronal MRI.
CATEGORY: BRAIN // CYSTIC MENINGIOMA
55 year old woman with balance problems and a large left frontal mass / Cystic Meningioma
This is a 55 year old right-handed woman who was having progressive balance problems. MRI with and without contrast demonstrated a 7 cm partly cystic meningioma involving the left frontal convexity and falx, and encasing the superior sagittal sinus. There was also tumor involvement of part of the convexity skull.
Meningiomas are common benign brain tumors. When they are of small to medium size, observation or stereotactic radiosurgery may be the most reasonable options. Large tumors may require open surgery.