- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
Non-Fusion Alternative for Treating Adjacent Segment Disease
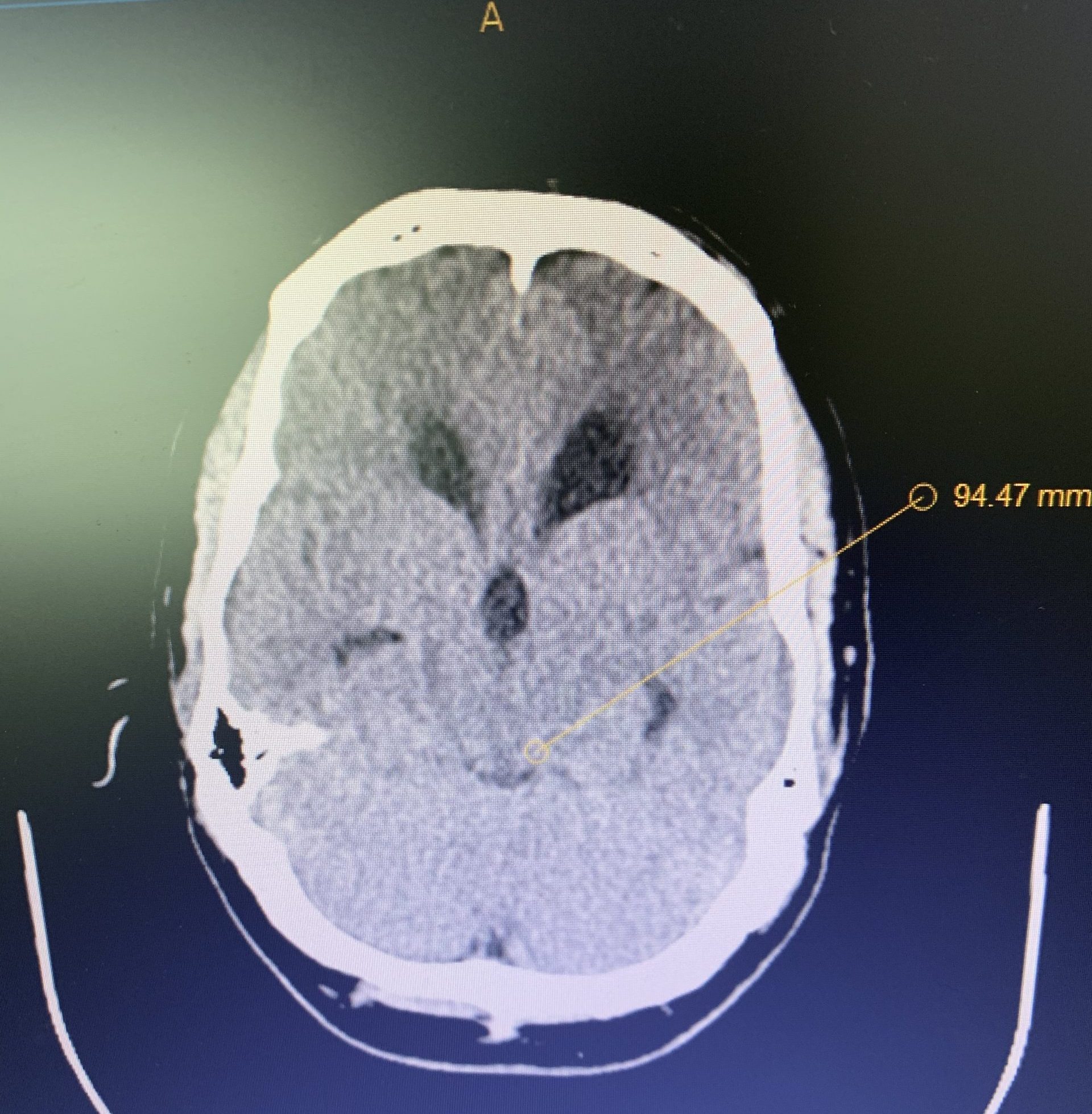
Hydrocephalus and Brainstem Tumor
April 8, 2022
Unusual Indication for Carotid Stenting Over Endarterectomy
May 2, 2022This is a 42-year-old otherwise healthy male who presented electively with progressively worsening neck pain radiating down the left arm, with paresthesia first three digits. He had a previous C6-7 anterior cervical discectomy and fusion (ACDF) two years prior, for which he recovered well. He was referred to Dr. Xavier Gaudin for a neurosurgical spine evaluation. An MRI cervical spine was obtained, which demonstrated C5-6 adjacent segment degenerative disease with a large disc extrusion resulting in severe left lateral recess and foraminal stenosis (Figure 1).

Figure 1: Preoperative MRI demonstrating C5-6 disc herniation with stenosis, adjacent to the previous C6-7 ACDF.
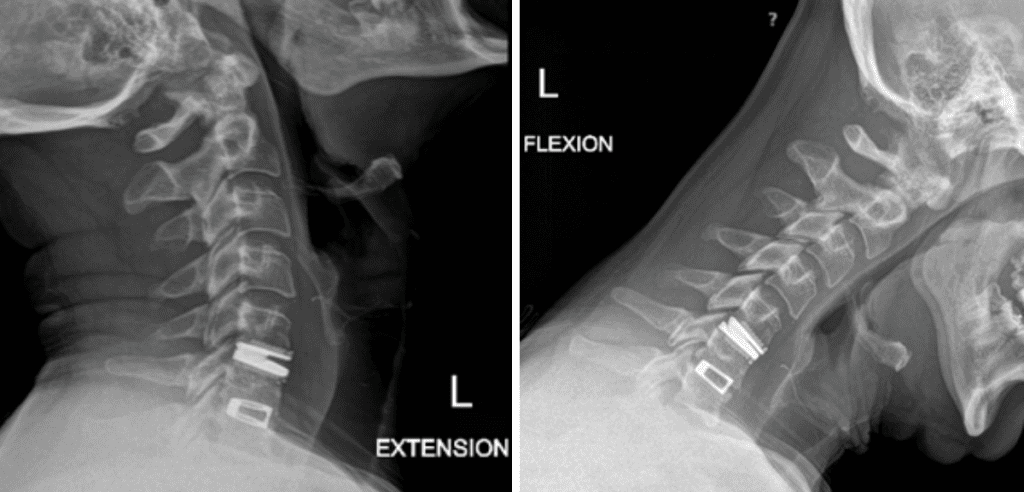
He had no neurologic deficits on exam, and therefore was started on a trial of multidisciplinary and multimodal conservative management. This included non-opioid pharmacologic regiment, lifestyle modification, physiotherapy, chiropractic, and epidural steroid injection. Despite these conservative measures, his symptoms remained severe and debilitating, and therefore surgical options were discussed. He underwent an uneventful C5-6 anterior artificial disc replacement. Postoperatively, his neck and radicular arm pain had fully resolved. Imaging demonstrated maintained physiologic flexion and extension of the cervical spine (Figure 2). This motion-preserving surgery reduces the adjacent degeneration process, and the need for further surgeries down the line.
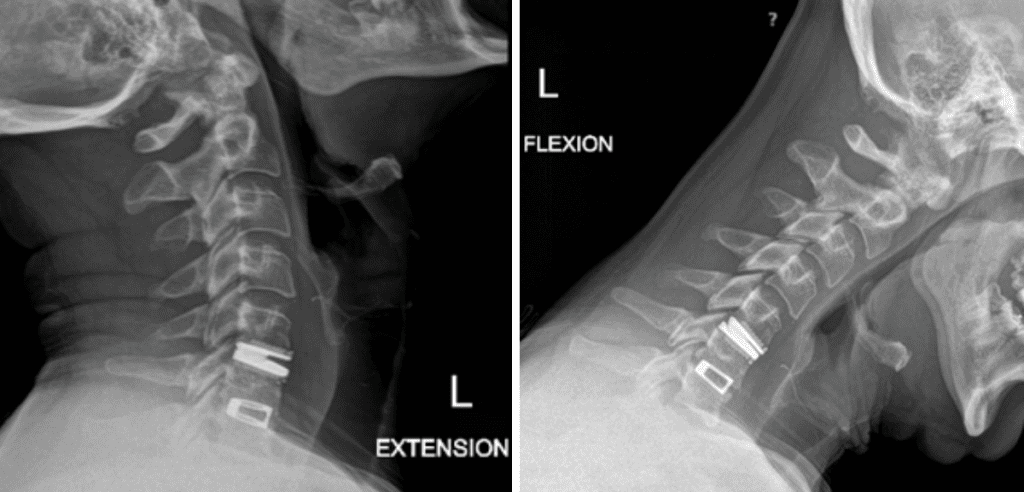
Figure 2: Postoperative dynamic xrays; note the differences in range of motions between the artificial disc at C5-6 and the previous fusion at C6-7.
Artificial cervical disc replacement, also known as total disc replacement or arthroplasty, allows for preservation of spinal range of motions. This non-fusion alternative reduces the biomechanical stress on the adjacent segments of the spine, which decreases the rate of physiologic degeneration cascade. The prevalence of adjacent segment degeneration after a spinal fusion is about 15%. In addition, artificial disc replacement does not require postoperative collar immobilization, thereby allowing for the patient to return to work and their usual activities sooner than a fusion. It may also be a better option for patients who are at risk of fusion failure (i.e. pseudoarthrosis), such as diabetics and nicotine users. While the current FDA guidelines and indications for artificial cervical disc replacement are limited, there are several off-label uses that are well supported in the literature. Under the care of a complex spine professional, artificial disc replacement can be utilized to treat adjacent segment disease, multilevel disease (greater than 2 segments), pseudoarthrosis, and even reversal of previous spinal fusion.
References:
Xu S, Liang Y, Zhu Z, Qian Y, Liu H. Adjacent segment degeneration or disease after cervical total disc replacement: a meta-analysis of randomized controlled trials. J Orthop Surg Res. 2018;13(1):244. Published 2018 Oct 3
Patwardhan AG, Havey RM. Biomechanics of Cervical Disc Arthroplasty-A Review of Concepts and Current Technology. Int J Spine Surg. 2020;14(s2):S14-S28
Gornet MF, Schranck FW, Sorensen KM, Copay AG. Multilevel Cervical Disc Arthroplasty: Long-Term Outcomes at 3 and 4 Levels. Int J Spine Surg. 2020;14(s2):S41-S49. doi:10.14444/7090
CATEGORY: SPINE // NON-FUSION ALTERNATIVE FOR TREATING ADJACENT SEGMENT DISEASE
Non-Fusion Alternative for Treating Adjacent Segment Disease

Authors
To learn more about the author, click his name or photo:
