- PATIENT FORMS | REQUEST A CONSULTATION | CONTACT US
- 1-844-NSPC-DOC
Spinal Cord Compression In Obese Patient
Severe Stenosis With A Grade 1 Spondylolisthesis
May 11, 2022
72-Year-Old Male With Progressive Neck Pain
May 11, 2022
IMG 5140 768x1024 1
Patients who are morbidly obese are particularly challenging to manage with spine pathology. When these patients have low back pain and concurrent severe lumbar degeneration, it is difficult to determine if their back pain is caused by their weight or MRI findings. In patients who have surgery for axial low back pain who have fusion surgery, it may be unrealistic to believe their pain will be improved unless they have severe lumbar stenosis as well as leg symptoms. In that case it is clearer cut and more likely to be successful. However, the surgical approach is very difficult not only to get exposure, but also because of the depth of the exposure there is a limitation because of the length of the instruments and the angles that need to be used to accomplish surgical goals.
In the cervical spine the success of relieving signs and symptoms may be greater if the patient has excellent correlative findings on the MRI with their symptoms and exam This is because the patient’s weight is not as much a variable in the cause of their neck pain. In general the success rate of operating on any patient whether they are overweight or not for purely axial neck pain with degenerative disc disease is not as high as with those patients with concurrent radicular pain, weakness, or signs of spinal cord compression which is called cervical myelopathy. Again it is very important that the symptoms correlate with the MRI.
In the case of an obese patient who requires an anterior cervical discectomy for either a soft herniated disc or a hard osteophyte, the surgical approach is challenging. Once exposure is obtained down to the disc space the surgery proceeds like any other case with a patient with a normal habitus. It is important to place the patient in good extension with an adequate roll under their scapula. It is helpful to tape down and stretch the excess tissue under the chin to the chest that allows a flatter surgical field. Although one has to use longer retractor blades sometimes it becomes easier to expose because there is often less strap muscle mass. Obese patients after surgery may require more monitoring particularly if they have sleep apnea or diabetes, but in general heavy patients do just fine if they their surgery is well indicated. They just need to understand the risks and limitations.

Figure 1: Sagittal T2-weighted MRI demonstrating a kyphotic cervical spine with C4-6 disc collapse with anterior osteophytes causing cord compression

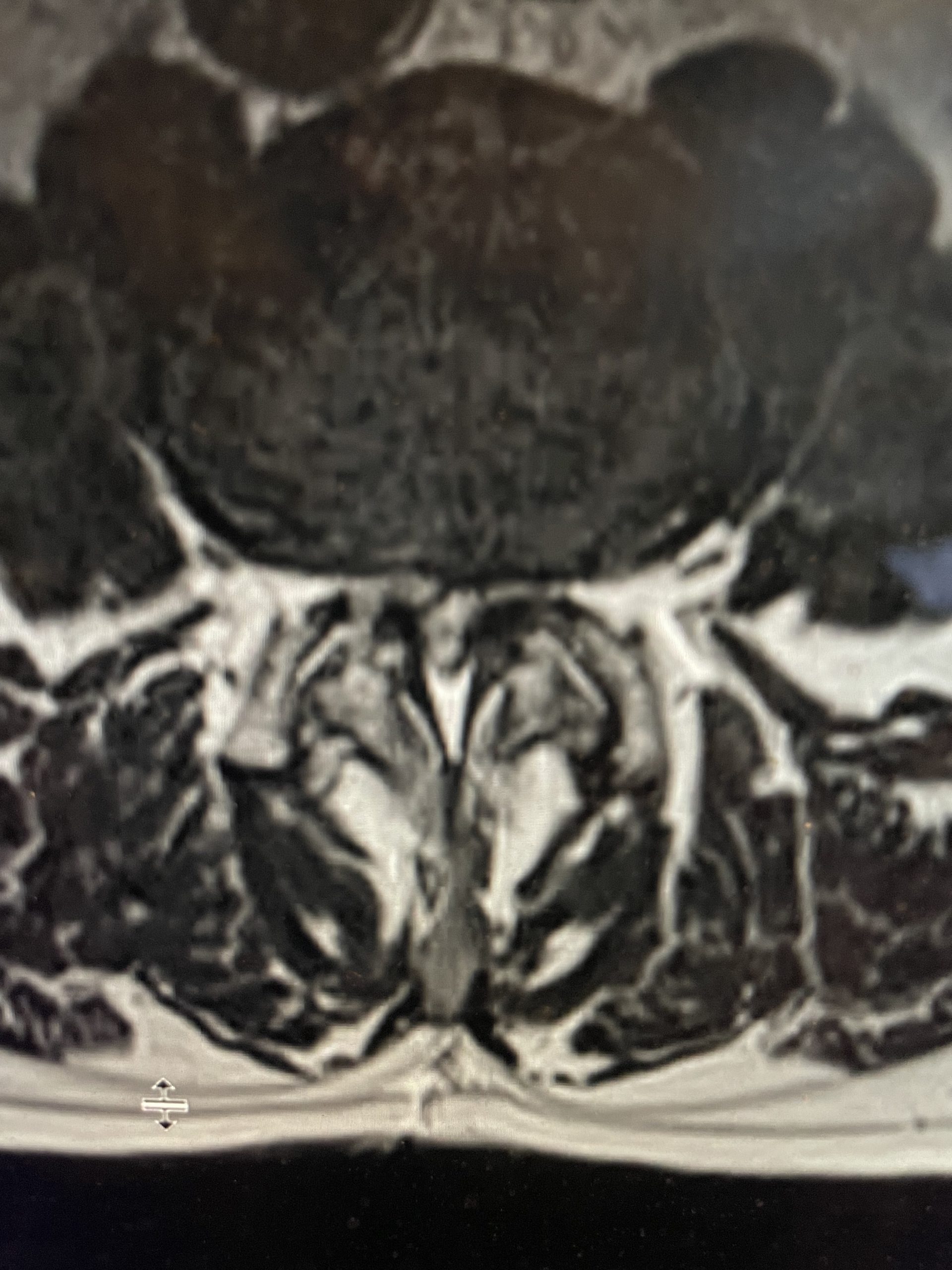
Fig 2: Axial T2-weighted MRI showing a large anterior osteophyte at C4-5 causing right greater than left spinal cord compression
Here is the case of a 51 year-old female who had a ten year history of severe neck pain with severe right arm pain, numbness, and weakness. She weighed over 300 pounds. She had failed all means of conservative management including medicines, physical therapy, chiropractic care, and epidurals. MRI demonstrated a reverse of the normal curvature of the cervical spine with large disc osteophyte complexes compressing the spinal cord (Fig 1). The C4-5 disc osteophyte was larger causing severe anterior compression of the spinal cord, worse on the right side (Fig 2). This correlated with the patient’s clinical findings. Therefore surgery was recommended. Patient underwent an anterior cervical discectomy and fusion with a plate from C4-C6. We were able to get her into a good position. Although there was a very deep exposure through the fat layer, it was not too bad to expose the face of the spine (Fig 3). Because there is less muscle, tissue planes open up actually easier sometimes particularly in women because of a relative decrease in muscle mass. The same goes for exposure of the lumbar spine. The majority of “herniated discs” in the cervical spine are actually bony protrusions we call osteophytes. After you clear away all the other cartilage that is the soft part of the disc, the way to get rid of that C4-5 osteophyte which acts like a sheet of bone at the posterior aspect of the disc space, is to drill it down to a fine shell and remove it with a special tool. This tool is called a Kerrison and has a very thin footplate that allows a plane between the osteophyte and dura which is being compressed and bites away this bone. The patient had good relief of her symptoms postoperatively.
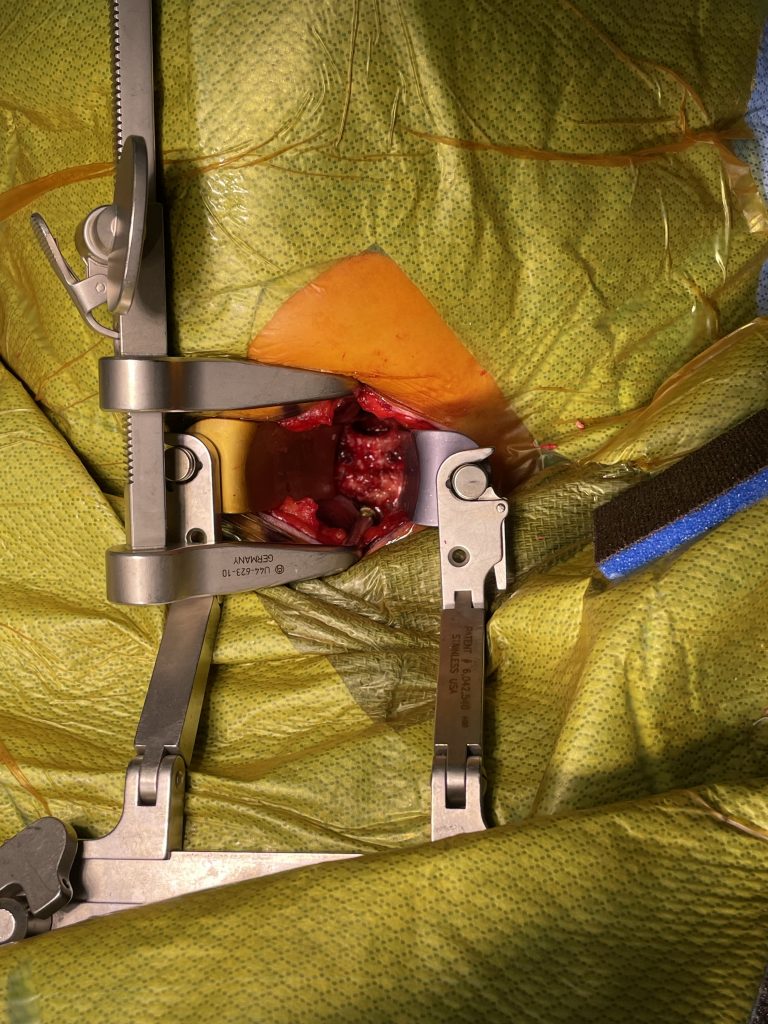
Fig 3: Intraoperative photo showing a deep exposure with deep retractors to access the anterior cervical spine

